Evaluation of Anti-Toxoplasma IgG, IgM, and IgA in Mothers with Spontaneous Abortion in Zanjan, Northwest Iran
Article information
Abstract
Toxoplasma gondii is one of the major agents of infectious abortions and due to its worldwide distribution can threat healthy pregnant women who had no previous exposure to this parasite. The present study was designed to investigate the contribution of T. gondii to spontaneous abortions in Zanjan, Northwest of Iran, using ELISA method. Blood Samples were collected from 264 mothers referred to the provincial hospitals of Zanjan due to spontaneous abortion. The sera were isolated and subjected to evaluate the anti-Toxoplasma IgG, IgM and IgA antibodies. The results showed IgG positive (IgG+) in 99 cases (37.5%). A total of 68 women (25.8%) showed seroconversion with IgM or IgA or both IgM and IgA. They included: IgM+ in 21 (8.0%), IgA+ in 23 (8.7%) and both IgM+ and IgA+ in 24 (9.1%) subjects. In 23 cases, positive titers of IgM and IgG were accompanied. In general, the analysis of anti-Toxoplasma antibody patterns, showed that about 17% of the spontaneous abortions were associated with serological patterns of acute infection. According to these findings, a considerable proportion of spontaneous abortions can be attributed to T. gondii in the study area.
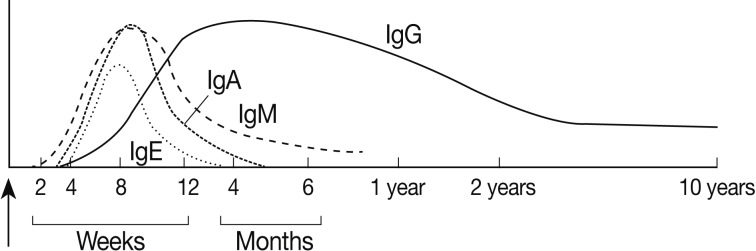
Toxoplasmosis is one of the most common parasitic infections distributed worldwide. Its prevalence varies in different regions [1], ranging between <1 to >80% [2]. Based on several studies in Iran, the seroprevalence of Toxoplasma gondii has been found to be 12.8% up to 86.3% in different regions. A combination of anti-Toxoplasma antibodies (IgM, IgG, IgA, and IgE) assay is one of the most useful tools for the diagnosis and identification of different phases of toxoplasmosis. Development of different antibodies during different phases of the infection, which is the basis of the above diagnostic assay, has been diagramed in Joynson and Guy [3] (Fig. 1).
Congenital toxoplasmosis, as one of the major clinical outcomes of Toxoplasma infection, occurs in women who have not experienced previous exposure to the parasite. This infection has been shown as one of the most important causes of spontaneous abortions, stillbirths, and premature deliveries [4]. In 1978, a study on 152 women with spontaneous abortion using hemagglutination (HA) and immunofluorescence antibody (IFA) assays showed 40.8% and 38.2% positive cases of toxoplasmosis, respectively [5]. In another study in France, out of 272 cases of congenital toxoplasmosis, 11 cases with termination of pregnancy, including 6 abortions and 5 fetal deaths were reported [6].
Two studies focusing on Toxoplasma seroprevalence in pregnant women in Zanjan Province were previously performed. Anti-Toxoplasma IgG, indicative of prior infection, was found in 47.3% in one study [7] and 37.8% in another [8]. They found quite few cases of IgM seropositives. The IgG positive rates imply that T. gondii is abundant in this region, and at the same time, more than a half of the pregnant women were not immunized, being at risk of exposure and consequent infection during pregnancy.
According to the medical records in the study area, only in one of the provincial major hospitals, about 30 cases of spontaneous abortion have been referred monthly. Despite the occurrence of a considerable number of abortions and loosing fetuses, no data about the infectious causative agents have been documented. Therefore, the present study was designed to investigate the possible involvement of T. gondii infection in spontaneous abortions in this region by serodiagnosis of anti-Toxoplasma IgM, IgG, and IgA antibodies.
In this cross-sectional study, 264 women with spontaneous abortion, referred to the hospitals of Zanjan Province, Northwest of Iran, were subjected to the investigation. Blood samples, 4 ml each, were collected immediately after the abortion. Generally, the women with the occurrence of abortion in gestation age lower than 20 weeks were selected and non-spontaneous abortion cases were excluded. Samples were transferred to the research laboratory of the Department of Parasitology at Zanjan University of Medical Sciences, Zanjan, Iran. Also, questionnaires, including personal information (age, residential place, parity, trauma experience, gestation age, and history of previous abortion) were filled in by experienced nurses. The research proposal was approved by the Research Ethics Committee of the University (reference number: 88-5-310) with the condition of taking informed written consent from the subjects for blood sampling and information collecting. Sera were isolated and kept in sterile microtubes at -20℃ until use for serological examinations. The ELISA kits (EUROIMMUN®, City Name, Germany) were used for the evaluation of anti-Toxoplasma IgG, IgM, and IgA antibodies.
The studied subjects (264 women), included 72% urban and 28% rural residents, with mean age of 28.6 years and minimum and maximum of 14 and 57 years, respectively. Most of them (76.5%) had no prior history of abortion. Anti-Toxoplasma serology showed IgG positive (IgG+) in 99 cases (37.5%). A total of 68 women (25.8%) showed seroconversion either with IgM or IgA or both IgM and IgA. IgM was positive in 21 (8.0%), IgA in 23 (8.7%), and both IgM and IgA were positive in 24 (9.1%) subjects. In 23 cases, positive titers of IgM and IgG were accompanied. The observed serologic patterns are detailed in Table 1.
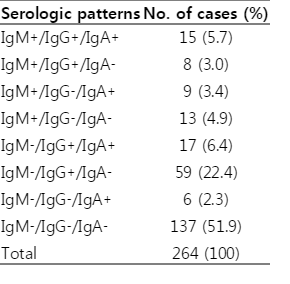
Serologic patterns of IgM, IgG, and IgA anti-Toxoplasma antibodies observed in women with spontaneous abortion in Zanjan, Northwest Iran
This study demonstrated that about 17% of cases with spontaneous abortions in Zanjan were associated with one of the serological patterns of acute toxoplasmosis. The results are interpreted according to the time course of immunoglobulin responses to T. gondii (Fig. 1). Fifteen patients (5.7%) were found to have IgM+-IgG+-IgA+ pattern indicative of relatively recent exposure to T. gondii. In these cases, IgG was also developed, thus, the time of infection was likely between 8 to 12 weeks, and involvement of Toxoplasma infection was possible. With the pattern of IgM+-IgG+-IgA-, 8 women (3.0%) were found. In these cases, the presence of IgG with no significant titers of IgA confirmed that the infection was not very recent. In cases with both IgM and IgG positive conditions, the infection is supposed to be older than 5 to 6 months and is unlikely to cause toxoplasmic abortion. However, other aspects (e.g., identifying possible changes in IgG and/or IgM titers) and alternative diagnostic techniques are recommended to consider for a better resolution in such cases.
The pattern of IgM+-IgA+-IgG- was seen in 9 patients (3.4%), indicating acute infections with estimated time course of 8 weeks. Observation of only IgM antibody (in IgM+-IgG--IgA- pattern) in 13 patients (4.9%) implies a very recent infection (less than 4 weeks) in these cases. Abortion in these 2 groups is most probably due to T. gondii.
The serologic results of 17 women (6.4%) were matched with the pattern of IgM--IgG+-IgA+. Although this pattern seems to be irregular, a new study in mice which had chronic toxoplasmosis showed that proliferation of tachyzoites in case of reactivation of Toxoplasma infection may increase IgG and IgA but not IgM [9]. Hence, this could be proposed with these 17 cases but more evaluations can be helpful to further clarify such serologic conditions. In 59 (22.4%) cases with the pattern of IgM--IgG+-IgA-, no T. gondii could have been responsible for the abortion. Six subjects (2.3%) showed IgM--IgG--IgA+ pattern. A variety of description could be proposed, i.e., IgA false positive, IgM false negative, or a correct IgA response appearing earlier than the IgM response. Therefore, Toxoplasma involvement in these cases is not known. Finally, a large number of women, 137 (51.9%) showed the pattern of IgM--IgG--IgA-, indicating no exposure to Toxoplasma parasite. These women are at risk of acute toxoplasmosis in any time and were advised to take care of their next pregnancy.
A limited number of studies considering Toxoplasma involvement in abortion have been performed with different design from our study and cannot be challenged with the present findings, an example of which is a study by Lolis et al. [5] on 152 women with spontaneous abortion. They found 40.8% and 38.2% Toxoplasma seropositive by hemagglutination and immunofluorescence antibody assays, respectively, but they did not present clear differentiation between acute and latent infections. In a study in Kashmir in 1998, almost a half of the women who experienced recurrent abortions were reported to be positive for anti-Toxoplasma IgM [10]. We found no significant difference between these 2 groups (the groups with and without history of abortion) in distribution of anti-Toxoplasma antibody patterns. Repeated abortion is unlikely to be caused by T. gondii in immunocompetent mothers, as possible previous exposure cannot persist acutely for a long course and supposed to cause concomitant immunity. Another study in France surveyed 272 cases of congenital toxoplasmosis and reported 11 cases with termination of pregnancy [6].
It should be noted that, in general, default in serological methods like other diagnostic techniques is inevitable though concordance between serologic and molecular techniques (real-time PCR) was confirmed in a recent assay by Pignanelli [11]. Also, further serologic conditions like reinfection with a different parasite genotype [12], seeking resolution, may be involved. It is also noteworthy that as Toxoplasma infections mostly occur without clinical symptoms due to infections with avirulent variants (genotype II), risk of a silent infection and passing to the fetuses is high. Among the identified genotypes of T. gondii, type II is found to be more frequent in pregnant women and other cases [13-15]. Based on a few studies in Iran [16], it has been demonstrated that genotype II is the dominant type existing in this region. So, characterization of parasite genotypes in all geographical regions is of other important baseline information required with regard to congenital toxoplasmosis and abortion consequences.
According to these findings, a considerable proportion of spontaneous abortions can be attributed to T. gondii in the study area. On the other hand, more than a half of the studied women had no history of T. gondii exposure and remain sensitive to toxoplasmosis. Serologic check up before and during pregnancy for the seronegative women is recommended.
ACKNOWLEDGMENTS
This study was supported by Zanjan University of Medical Sciences and Health Services, Zanjan, Iran. Abbas Amin was awarded by the university for his M.Sc. thesis. We thank all the staff at Obstetrics and Gynecology Departments of Ayatolah Musavi Hospital and Imam Hossein Hospital for their kind cooperation and collecting samples.