Comprehensive Review of Ocular Angiostrongyliasis with Special Reference to Optic Neuritis
Article information
Abstract
Angiostrongyliasis, caused by Angiostrongylus cantonensis infection, is a food-borne parasitic disease. Its larvae evoke eosinophilic inflammation in the central nervous system, but can also cause pathological changes in the eyes. Among ocular angiostrongyliasis cases, the incidence of optic neuritis is low and only few sporadic reports exist. Some patients with optic neuritis developed obvious hypopsia or even vision loss, which would seriously influence the quality of life of patients. Prompt treatment of optic neuritis caused by A. cantonensis is the key factor for minimizing the incidence of serious complications of this disease. In this review, we first provide a comprehensive overview of ocular angiostrongyliasis, and then focus on the clinical features of optic neuritis caused by A. cantonensis.
INTRODUCTION
Angiostrongyliasis caused by infection with Angiostrongylus cantonensis is primarily characterized by eosinophilic meningitis, meningoencephalitis, or myelitis [1]. Ingestion of raw or half-cooked apple snails containing third stage larvae (L3) of A. cantonensis is the commonest route of infection. After ingestion by humans, the L3 migrate to the central nervous system (CNS) via blood stream and cause eosinophilic meningitis, often associated with encephalitis and myelitis (meningo-encephalo-myelitis) [2]. At the same time, the larvae also can invade the eyes and cause various ocular symptoms including optic neuritis [3]. Ocular angiostrongyliasis, however, has been neglected due to its low incidence.
CURRENT STATUS OF OCULAR ANGIOSTRONGYLIASIS
Recently Diao et al. [3] summarized a total of 35 cases of ocular angiostrongyliasis. We also made an extensive literature survey on ocular angiostrongyliasis and found 42 cases including the cases reviewed by Diao et al. [3]. Of these, nearly a half (19 cases) were from Thailand [4-13], including the first case report from that country in 1962 [4] and the most recent case reported in 2013 [13]. There are a few sporadic reports of ocular angiostrongyliasis from other countries, mostly from Asia. We have found 5 cases from Sri Lanka [14-18], 2 [14,15] of which were cited by Diao et al. [3]. Two cases were reported from India [19,20]. Although Diao et al. [3] noted 3 cases from India, they mistakenly included 1 case from Taiwan (their reference #17, in our reference #25) as an Indian case. Four cases have been reported from mainland China [21-24] and 2 cases from Taiwan [25,26]. Among them, 1 case from Taiwan [25] was not cited in the review of Diao et al. [3]. Two cases from Japan [27,28] were both found in Okinawa Prefecture. One case from Vietnam [29] was not included in the list of Diao's cases [3]. One case each was reported from Indonesia [31], Papua New Guinea [32], Malaysia [33], South Africa [34], Nepal [35], and Jamaica [36], in the order of the reported year. The cases from Malaysia and Jamaica were not mentioned in the review of Diao et al. [3]. The case from Malaysia [33] was reported as an ocular gnathostomiasis. However, the picture provided in the publication [33] shows that the worm is definitely not a Gnathostoma larva: the body is filariform without an apparent head bulb, indicating that this worm is highly likely to be the larva of A. cantonensis.
All 42 cases of ocular angiostrongyliasis are listed in Table 1. Among them, the oldest records were reported by Joseph [37] and Nicholls [38] in Sri Lanka in 1925 (redescribed by Dissanike and Cross in 2004 [15]). The most recent one was the optic neuritis case reported from Khon Kaen, Thailand, by Sinawat et al. [13] in 2013. Except for the case from Jamaica [36], 41 out of 42 were recorded in Asia, corresponding to the geographical distribution of this parasite. Among 42 ocular angiostrongyliasis cases, 19 were from Thailand, 5 from Sri Lanka and only 1 or 2 cases from other countries. Since 47% of all angiostrongyliasis cases in general are from Thailand and 27% from China [1], a high prevalence of ocular cases in Thailand is to be expected. However, the low number of ocular cases reported from other countries in the region is unexpected. Given the low frequency of the condition even in Thailand, cases elsewhere might not be diagnosed correctly. Alternatively, there might be an intra-species variation in the pathogenicity and behavior of the L3 in the host. Related to this, genetic variation in relation to the geographic location of A. cantonensis has been reported [39].

Comprehensive review of the clinical features of ocular angiostrongyliasis cases in the world.
In addition to the sporadic cases listed in Table 1, Punyagupta et al. [40] analyzed clinical features of 484 cases of typical eosinophilic meningitis and found that 16% of patients had visual impairment, while 12% had an optic disc abnormality such as papilledema or atrophy. In China, clinical features of angiostrongyliasis cases of an outbreak in Wenzhou were analyzed [41] and the ocular manifestation was listed as one of the major features [42]. Ocular angiostrongyliasis cases were described also in recent reports of angiostrongyliasis outbreaks in China. Lv et al. [43] reported 2 ocular cases among 33 angiostrongyliasis cases in an outbreak in Dali. Wang et al. [44] reported 16 cases of visual disorders with different degrees of severity, such as photophobia, blurred vision, diplopia, defect in the field vision and eye floaters out of 81 cases in an outbreak of angiostrongyliasis in Beijing. In this outbreak, 25 patients showed severe symptoms and all ocular cases were found in this group. These reports indicate that the actual incidence of ocular angiostrongyliasis is likely much higher than commonly appreciated.
CLINICAL FEATURES OF OCULAR ANGIOSTRONGYLIASIS
The average age of the patients in 39 cases was 34 years (3-72 years), and unknown in the remaining 3 cases. There was an obvious sex difference (28 males, 12 females, and 2 unknown). Except for 1 case from Taiwan [26], all patients were affected only in 1 eye with no significant difference for the frequency of the affected sides (22 left and 19 right, including a case of bilateral necrotizing retinitis, data not available for 2 cases). In most instances, worms were found and surgically removed from the anterior chamber (14 cases) or from vitreous fluid (15 cases). In 10 cases, worms were found either on the retina or sub-retina. Even in such retinal involvement cases, worms were successfully removed surgically. In 4 retinal involvement cases in Thailand, laser ablation with or without oral steroids was successfully performed [11]. Among 30 cases of successful surgical removal, only 1 recorded the presence of 2 worms. In all other cases, ocular lesions seemed to be caused by a single worm. These ranged in length from 5 to 28 mm, but the majority was juveniles (young adults) around 10 mm long. The majority of ocular cases was not associated with CNS symptoms. Among the 42 ocular cases, only 12 patients were also suffering from eosinophilic meningitis. Peripheral blood eosinophilia was noted in 11 cases and 6 of them were among the cases with CNS symptoms.
OPTIC NEURITIS AND OTHER OCULAR ABNORMALITIES
Among 42 cases of ocular angiostrongyliasis, 6 were diagnosed as optic neuritis. The very first report of optic neuritis due to A. cantonensis infection described a case from China [22]. Subsequently, 4 cases have been reported from Thailand [12,13] and 1 case from Taiwan [25].
The diagnosis of optic neuritis can be made clinically by visual symptoms, positive rapid relative afferent pupillary defect (RAPD), and prolongation of visual evoked potentials (VEP) [45,46]. In the first A. cantonensis infection-associated optic neuritis case from China [22], the patient complained of mild headache, a low-grade fever, and slight ataxia. At the beginning, this patient was treated as a case of influenza because of non-specific symptoms, but A. cantonensis infection was suspected after the sudden onset of retinal detachment. The definite diagnosis was made by surgical removal of the worm.
The first angiostrongyliasis-associated optic neuritis case in Thailand [11] was a 21-year-old man suffering from progressive headache for 2 weeks. Repeated lumbar puncture could not relieve his headache and a week later he developed blurred vision in his left eye. The RAPD of his left eye was positive and VEP showed prolonged latency for this eye. Angiostrongylus worm was found in the vitreous space and treated with the argon laser.
In 2008, Sinawat et al. [12] studied 3 cases of optic neuritis caused by A. cantonensis. In all 3 cases, the fundus examination revealed generalized retinal pigment epithelial alteration, subretinal tracks, retinal edema, macular edema. and a pale disc, suggesting optic neuritis. In the first case, the patient, a 47-year-old man, complained of blurred vision in the left eye but denied headache. The latent phase of VEP was prolonged but the amplitude was normal. The RAPD of the left eye was positive and visual acuity was 1/60. Antibodies against the 29 KD antigen of A. cantonensis were detected in the serum. An immature male worm in the anterior chamber was aspirated by simcoe cannula after laser photocoagulation. The second case was a 27-year-old man presented with progressive visual loss in the left eye for 3 weeks. He presented with a 2-month history of eosinophilic meningitis before the onset of blurred vision. A moving larva was found in the superotemporal area of the vitreous humor. Diode laser was directly applied to the parasite and the dead worm was surgically removed. The third case was a 36-year-old man who developed visual loss in his right eye for 1 week without any history of headache. In this case, the intraocular inflammation was not detected and the RAPD was negative. The electroretinogram and VEP were normal. A subretinal living parasite was treated with a diode laser. His visual acuity was not much improved because of the retinal pigment degeneration.
Sinawat et al. [13] reported an additional ocular angiostrongyliasis case with retrobulbar optic neuritis. The patient was a 27-year-old Thai male presenting with progressive visual loss and a membrane-like floater in the right eye that had persisted for 1 month. The patient had a positive RAPD and delayed VEP in his right eye. The parasite found in the subretinal space was treated with a diode laser and surgically removed.
A case of optic neuritis reported from Taiwan was a 38-year-old man who suffered from headache and neck stiffness with blurred vision and color blindness in the left eye associated with binocular horizontal diplopia. The optic neuritis was confirmed by having a positive RAPD and delayed VEP in his left eye. The patient received larvicidal drugs and steroid treatment for 2 weeks, and his visual accuracy and color sense in the left eye were improved. As an overview (Table 2), all optic neuritis patients were males. Two cases in Thailand were affected in the right eye and the other 4 in the left eye. Unlike other infectious causes of optic neuritis [47,48], optic neuritis associated with ocular angiostrongyliasis is almost always unilateral. It may occur with or without eosinophilic meningitis or blood eosinophilia. Two of 6 cases had preceding meningitis. If both conditions coexist, eosinophilic meningitis will occur prior to optic neuritis or ocular involvement based on its life cycle. The larvae migrate to the meninges prior to randomly migrating to other tissues [1]. The postulated mechanism for optic neuritis is an increased intracranial pressure [25] or direct invasion [49]. In 2008, Jin et al. [49] performed MRI examinations for 74 angiostrongyliasis patients and found 33 with abnormal MRI including 1 optic neuritis case. In this optic neuritis case, a nodular lesion was observed on the optic nerve by the brain MRI. Related to this, optic nerve compression due to A. cantonensis was also reported from China [24].
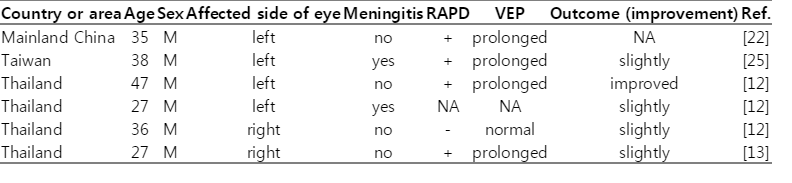
Reported cases of optic neuritis due to A. cantonensis infection
Ocular involvement other than optic neuritis in angiostrongyliasis included blepharospasm, uveitis, macular edema, retinal edema, necrotic retinitis, panophthalmitis, papilledema, and optic nerve compression. In the case of necrotic retinitis reported from Taiwan [25], the patient had sudden loss of vision in both eyes and yellow transudate of retina accompanied by bulla formed by bilateral retinal detachment. Both serum and cerebrospinal fluid were antibody-positive against A. cantonensis by ELISA, and serum and subretinal fluid were positive for A. cantonensis by western blotting [25].
DIAGNOSIS, TREATMENT, AND PROGNOSIS OF OPTIC NEURITIS CAUSED BY A. CANTONENSIS
The most common diagnostic method for optic neuritis caused by A. cantonensis infection is ophthalmological examination (ophthalmoscope, ERG, and VEP). Furthermore, inquiry of history of eating intermediate hosts of A. cantonensis is also a key for diagnosis. Immunodiagnosis, including ELISA, western blotting, and use of specific monoclonal antibodies, provide strong supportive evidence. Peripheral blood eosinophilia is also indicative. The most reliable diagnostic method so far is to find put larvae or juveniles of A. cantonensis by ophthalmoscopy.
The usual method of treatment of optic neuritis caused by A. cantonensis is surgical removal of the parasites. If the parasites have not yet caused tissues damage, laser-mediated killing of living worms is a recommended therapeutic measure, which is better than surgical removal. In addition, oral administration of steroids may improve visual acuity by reducing intraocular inflammation. Anthelmintics, such as albendazole, are not recommended because dead parasites may cause serious intraocular inflammation [11].
In spite of these therapeutic measures, the prognosis for optic neuritis caused by A. cantonensis is not favorable. As shown in Table 2, only slight improvement of visual acuity occurred after treatment in most cases. For both optic and general ocular angiostrongyliasis, the outcome of therapy depends on the duration of infection and the initial visual acuity at the first visit of patients to doctors [3].
PERSPECTIVES OF OPTIC NEURITIS CAUSED BY A. CANTONENSIS
Although the incidence of optic neuritis in A. cantonensis infection is far lower than that of eosinophilic meningitis, its poor prognosis in terms of vision loss seriously affects the quality of the life of patients. At present, we do not fully know the answers to the following questions:
How do larvae migrate into the eyes? Via blood flow or by other routes?
What is the relationship between optic neuritis and eosinophilic meningitis?
What is the relationship among clinical symptoms, pathological changes, and the prognosis? What causes those pathological changes?
How can we treat cases of optic neuritis due to A. cantonensis infection?
Because only a limited number of optic neuritis cases have been reported, development of an animal model for A. cantonensis-associated optic neuritis is necessary.
ANIMAL EXPERIMENTS FOR OPTIC NEURITIS CAUSED BY A. CANTONENSIS
In the past 20 years, many animal experiments have been carried out using rodent models of A. cantonensis infection [50]. Among them, mice have been studied most extensively because of their susceptibility to the parasite. Until now, however, there are no animal models for optic neuritis caused by A. cantonensis. Rats and mice have provided research models for optic neuritis caused by other conditions, such as multiple sclerosis. In these models, histopathological changes of the retina and optic nerve were observed by H-E staining, and demyelination of the optic nerve was observed by electron microscopy. Similarly, fundoscopy has been used to observe the damage to the optic papilla and ERG/VEP used to examine changes in vision and visual acuity. Ganglion cells of the retina were also the focal point of the study of optic neuritis [51,52]. Similar methodology should be adopted for the study of optic neuritis caused by A. cantonensis.
In our preliminary animal study using mice infected with A. cantonensis, we found the infected animals manifested obvious inflammatory infiltration in the retina and optic nerve, and demyelination was found in the optic nerve. Meanwhile, VEP and ERG were very different compared with normal control animals (unpublished results). These results indicate A. cantonensis can cause pathological and clinical changes of eyes in experimental animals.
In conclusion, ocular angiostrongyliasis was comprehensively reviewed with special focus on optic neuritis caused by A. cantonensis, and we put forward questions about the urgent problems which need to be solved. This study provides a baseline for future research on optic neuritis caused by A. cantonensis.
ACKNOWLEDGMENTS
This work was supported by a grant from the National Basic Research Program of China (2010CB530004), the National Natural Science Foundation of China (grant no. 81271855, 81261160324) and The PhD Start-up Fund of Natural Science Foundation of Guangdong Province of China (4203021) grant.