Determinant of parasite clearance and density on uncomplicated falciparum malaria infections in malaria-endemic area of Lampung Province, Indonesia
Article information

Abstract
Lampung is a malaria-endemic region in Indonesia with an annual parasite incidence of 0.06 per 1,000 population. The socio-demographic factors, clinical conditions, and artemisinin combination therapy (ACT) types might affect parasite clearance and parasite density. This study aims to investigate factors that influence parasite clearance and parasite density in malaria patients. A retrospective analytic observational and a cross-sectional approach was used to conduct this study. A total of 66 malaria patients were examined to investigate parasite density and clearance, socio-demographic profiles, clinical conditions, and ACT types. To analyze data, univariate, bivariate, and multivariate tests were used. Age (P=0.045; r=0.238) and ACT type (P=0.021; r=0.273) were the only variables that had a significant correlation with parasite clearance. Age (P=0.003; r=0.345) had a significant correlation with parasite density. The most influential factors related to parasite clearance were the ACT type (dihydroartemisinin piperaquine) (P=0.017; odds ratio (OR) 0.109; 95.0% confidence interval (CI), 0.018–0.675) and age (P=0.030; OR 0.132; 95.0% CI, 0.021–0.823). Age (P=0.046; OR 0.320; 0.105–0.978, 95.0% CI) was the most significant variable associated with parasite density.
Introduction
Malaria is a vector-borne disease and part of the indicators for sustainable development goals [1]. Based on the World Health Organization report, the malaria incidence rate was 59.2 per 1,000 population in 2021, which has increased compared to 2019 (57.2 per 1,000 population at risk). Global malaria mortality in 2021 was 14.6 per 100,000 population at risk, which has increased compared to 2019 (14.0 per 100,000 population at risk) [2]. Malaria-endemic areas in Indonesia have different levels of endemicity, where the annual parasite incidence (API) in 2021 has increased to 1.12 [3] per 1,000 population compared to 2019, which was 0.93 [1] per 1,000 population. Lampung Province is one of the malaria endemic areas in Indonesia, but API is currently declining. The API in 2021 was 0.06 per 1,000 population, meanwhile the API in 2019 was 0.19 per 1,000 population [4], where Pesawaran Regency still has the highest API value, which is 0.82 [4] per 1,000 population. This condition has decreased compared to 2019 (1.97 per 1,000 population) [5].
Malaria symptoms have a broad spectrum of clinical manifestations, such as asymptomatic, mild, uncomplicated, and severe complications. However, fever associated with headache, anemia, arthralgia, and other non-specific symptoms comprise the main symptoms of malaria infection [7–10]. These clinical manifestations are related to the parasite’s density, which increases with the degree of tissue damage, resulting in a more severe clinical condition [11]. Therefore, parasite density is directly proportional to the body’s level of response to infection. Moreover, when the liver schizonts and/or erythrocyte schizonts rupture, these symptoms manifest [10,12].
Moreover, the high parasite density at the initiation of the examination, antimalarial effectiveness, and presence of mutations affect the positive parasite rate on the third day after treatment. Also, effective antimalarial medications can greatly reduce the parasite density and provide symptom relief. According to several studies, the appropriate administration of artemisinin combination therapy (ACT) reduces parasitemia from the first day of treatment. Subsequently, fever lyses with the gradual resolution of other clinical symptoms. Currently, dihydroartemisinin piperaquine (DHP) plus primaquine, which has high efficacy, is the ACT type used in Indonesia. However, two types of medications in this class, including DHP and artesunate-amodiaquine-primaquine (AAQ), were previously used. Additionally, DHP is the first-line antimalarial drug used for standard malaria treatment, while AAQ is no longer used due to its decreasing effectiveness [13–15].
The study of socio-demographic factors, clinical conditions, disappearance time of clinical symptoms, and the ACT type, that influence parasite clearance and parasite density in malaria falciparum patients, is interesting. Therefore, this study aims to investigate factors that influence parasite clearance and density in malaria falciparum patients in the endemic area of Pesawaran Regency, Lampung Province, Indonesia.
Materials and Methods
This is a retrospective analytic observational and cross-sectional study, which was conducted in the malaria-endemic region of Pesawaran Regency, Lampung Province. The study population included malaria patients, who were treated at the Hanura Health Center in 2013. The calculated minimum number of samples was 61, with a 95.0% confidence interval (CI), relative accuracy of 10.0%, and 19.7% malaria incidence proportion [16]. The inclusion criteria are as follows: uncomplicated malaria cases, a single infection of Plasmodium falciparum based on thin smear of peripheral blood examination, age greater than 1 year old, and received ACT (DHP or AAQ) treatment. The presence of sexual stage on thin microscopic examination is the only exclusion criterion.
Serial data collection, microscopic examination, and clinical symptom assessment were conducted for 28 days at the Clinical Laboratory of the Hanura Health Center. The parasite density (parasitemia) was calculated per 200 leukocytes [17,18], while information on clinical symptoms was obtained through history taking and interviews using questionnaires. Social determinants of health data (age, gender, and occupation) were assessed through interviews (D0). Assessment of the disappearance time of clinical symptoms was performed by taking anamnesis or interviews, starting from D+1 after the first day of treatment until the 28th observation day. Also, the evaluation of parasite clearance was conducted by calculating the parasite density at each observation period according to the microscopic examination schedule.
Statistical tests were used for the data analysis to analyze univariate, bivariate, and multivariate variables. The median value, range, and percentage were used for the univariate analysis, while the contingency coefficient correlation test was used for the bivariate analysis. Contingency coefficient correlation test results were set with a P-value>0.25 followed by a multivariate test (logistic regression). IBM SPSS version 20 (SPSS, Chicago, IL, USA) was used for all statistical tests. The statistical test with a P-value<0.05 showed significant results. In this study, the operational definitions of the study variables and the type of correlation test used are shown in Supplementary Table S1. This study obtained ethical clearance approval from the Research Ethics Committee of the Faculty of Medicine, University of Lampung (number 1838/UN.26.18/PP.05.02.00.2021).
Results
Table 1 shows the profiles or characteristics of the study participants. The clinical symptoms of these individuals during their first treatment varied from mild, with only 1 symptom, to spontaneous bleeding, including signs of anemia (pale palpebral conjunctiva). The majority of the study participants (66.7%) presented with mild symptoms, which persisted briefly after treatment. Meanwhile, approximately 62.1% experienced resolution of the clinical symptoms after 3 days of therapy (late). In the calculation of parasite density, 50.0% of the participants had a value of <8,220 parasites/μl of blood (low), and 87.9% had a rapid (1–3 days) recovery based on the parasite clearance variable.
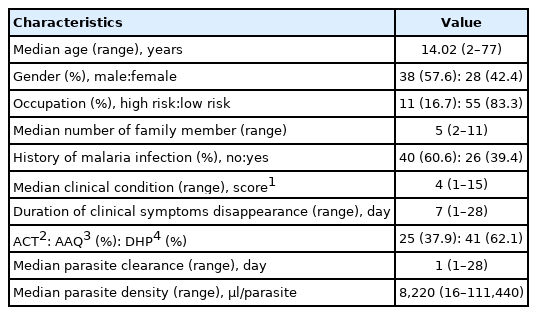
Characteristics of research subjects
Furthermore, Table 2 shows that bivariate analysis was used to determine the correlation of parasite clearance with various variables. Age (P=0.045) and ACT type (P=0.021) were significantly associated with parasite clearance. However, gender, type of occupation, number of family members, history of malarial infection, clinical conditions, duration of resolution of clinical symptoms, and parasite density had no significant correlation. A correlation between age (r=0.238) and ACT type (r=0.273) and parasite clearance was observed with weak strength, indicating a direct relationship between these variables.
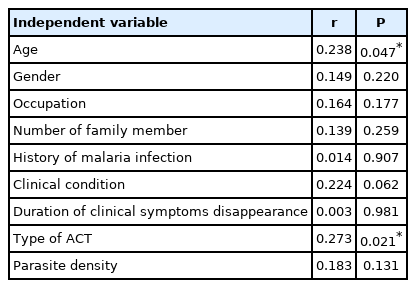
The correlation of age, gender, type of occupation, number of family member, history of malaria infection, clinical condition, duration of clinical symptoms disappearance, type of ACT and parasite density to parasite clearance
In Table 3, the bivariate analysis was used to determine the variables which correlated with parasite density. Age (P=0.003) and the type of occupation (P=0.003) have a significant correlation with parasite density, whereas there is no significant relationship between gender, number of family members, history of malarial infection, clinical condition, and duration of clinical symptom disappearance. The correlation strength between age (r=0.345) and type of occupation (0.344) and parasite density was moderate; hence, a direct relationship was observed between these variables.
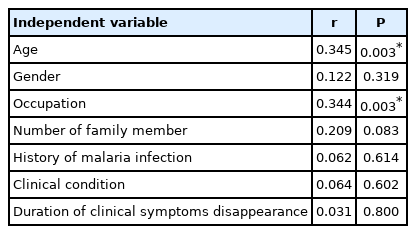
The correlation of age, gender, type of occupation, number of family member, history of malaria infection, clinical condition, duration of clinical symptoms disappearance to parasite density at the first came to the public health centre
The most influential factors related to parasite clearance included the ACT type (DHP) (P=0.017; odds ratio (OR) 0.109; 95.0% CI, 0.018–0.675) and age (P=0.030; OR 0.132; 95.0% CI, 0.021–0.823). To calculate the influence of the independent variables on parasite clearance, it is necessary to calculate the Y value first (Y=−0.096+(−2.024) (age)+(−2.215) (type of ACT)). After the Y value is obtained, the probability (p) of the effect can be calculated using the prediction model equation (P=1/(1+ey)). If the patient is an adult and receives DHP treatment, it will affect parasite clearance by 52.4%; however, if the child is treated with AAQ, it will affect parasite clearance by 98.7%.
Meanwhile, age (P=0.046; OR 0.320; 95.0% CI, 0.105–0.978) was the most dominant factor that correlated with parasite density. To predict the probability of the effect of the independent variable on the dependent variable (parasite density), the procedure is performed using the same method as before. The value of Y is calculated using the following equation: Y=−1.163+(−1.139) (age). If the patient is an adult, it will affect parasite density by 76.0%, whereas if the patient is a child, it will affect parasite density by 90.8%.
Discussion
Statistically, parasite clearance correlates with density, age, occupation, and ACT type. However, the most influential variables related to parasite clearance, the process of clearing parasites from the host after treatment with antimalarials, are the ACT type and age. The ability of antimalarials to kill these organisms is related to the parasite cleaning process, where a reduction in the clearance rate can be attributed to antimalarial drug resistance. Moreover, 3 aspects contribute to parasite clearance, including host defense mechanisms (immune response), antimalarial drug effects, and infection pathogenesis (sequestration) [19]. ACT rapidly decreases parasite density and clearance process after the first 6 h of administration and clearing up after 36 h in sensitive Plasmodium sp. strains [19]. The presence of polymorphisms in certain genes causes resistance to ACT, such as polymorphisms in the PfK13 (PF3D7_1343700; ID : 814205) [20], PfMDR (PF3D7_0523000; ID: 813045) [14], and other genes. However, another study reported a reduced parasite clearance in the absence of the K13 gene polymorphism. In that study, plasma concentrations of ACT decreased, especially in elderly patients; thus, a dose increase was required [20–22].
Furthermore, parasite clearance is influenced by its density, where a direct relationship exists between these variables. This finding was reported in previous studies, where the parasite density affected the clinical symptoms and was directly proportional to its clearance. However, another study elucidated that a reduction in parasite clearance was observed in severe malaria [10–12,20]. The type of occupation by the majority of the study population involved fishing, with a high risk of contracting malaria. Although the participants who had a risky occupation only comprised 16.0%, this factor was significantly associated with parasite clearance and density. In addition, when working at night, the risk of exposure to Plasmodium due to Anopheles mosquito bites is greater [23,24]. Therefore, the correlation between parasite clearance and the type of occupation depends on the density of the parasite, where a high concentration of the organism prolongs its clearance [10–12,20].
Bivariate analysis was also conducted to ascertain the correlation between parasite density and several variables. Consequently, age, clinical condition, and type of occupation were significantly associated with parasite density, where age was the most influential factor. These results are in accordance with previous studies, which stated that this variable had an inverse relationship with parasite density. Also, the immune response develops as the host matures and is strengthened with repeated exposure to the parasite [25]. Moreover, some factors influence parasite density, including the severity of malaria complications, transmission type, early diagnosis, adequate treatment, and the patient’s immune response [8].
Moreover, clinical conditions are usually related to living in areas with high malarial endemicity, parasite density, and infection quantity. In addition, the density of the parasite is directly proportional to the response level of the human body to infection. The process of schizont rupture occurs in the asexual parasite life cycle, which lasts between 24 h and 48 h depending on the Plasmodium sp. An increase in the parasite number due to the continuous cycle, until the threshold is exceeded, will induce clinical symptoms, especially fever. This phenomenon occurs due to the release of inflammatory mediators C-reactive protein and tumor necrosis factor-α (TNF-α). Furthermore, a non-specific natural immune response appears in the form of macrophage phagocytosis against parasites and infected erythrocytes during the first infection. This will trigger the release of inflammatory mediators TNF-α, interleukin 10, and interferon [10]. However, in repeated infections within highly endemic areas, specific antibodies and an immune response are formed, which control immunity. This immune response is more effective in eliminating parasites [11,12,25,26].
Supplementary Information
Acknowledgments
The authors are grateful to Prof. dr. Supargiyono, DTM&H., SU.,PhD., Sp.Par.K; Prof. drh. Widya Asmara, SU., PhD; Prof. dr. Hari Kusnanto, SU., Dr.PH. The authors are also grateful to the Government and Health Office of the Pesawaran District, Hanura Health Center, and all the participants, who participated in this study.
Notes
The authors have no conflicts of interest to declare.
Author contributions
Conceptualization: Suwandi JF, Kurniawan A, Susanto L
Data curation: Suwandi JF, Kurniawan A, Susanto L
Formal analysis: Suwandi JF, Kurniawan A
Funding acquisition: Suwandi JF
Investigation: Suwandi JF
Methodology: Suwandi JF, Kurniawan A, Susanto L
Project administration: Suwandi JF
Resources: Suwandi JF
Software: Suwandi JF
Supervision: Kurniawan A, Susanto L
Validation: Kurniawan A, Susanto L
Visualization: Suwandi JF, Kurniawan A, Susanto L
Writing—original draft: Suwandi JF, Kurniawan A, Susanto L
Writing—review and editing: Suwandi JF, Kurniawan A, Susanto L