A case of vocal cord gnathostomiasis diagnosed with sectional morphologies in a histopathological specimen from a Chinese woman living in Korea
Article information

Abstract
This study aimed to describe a rare case of gnathostomiasis in the vocal cord. A 54-year-old Chinese woman living in Korea visited with a chief complaint of voice change at the outpatient department of otorhinolaryngology in Hallym Sacred Heart Hospital, Hallym University on August 2, 2021. She had eaten raw conger a few weeks before the voice change developed, but her medical history and physical examinations demonstrated neither gastrointestinal symptoms nor other health problems. A round and red cystic lesion, recognized in the anterior part of the right vocal cord, was removed using forceps and scissors through laryngeal microsurgery. The histopathological specimen of the cyst revealed 3 cross-sections of a nematode larva in the lumen of the cyst wall composed of inflammatory cells and fibrotic tissues. They differ in diameter, from 190 μm to 235 μm. They showed characteristic cuticular layers with tegumental spines, somatic muscle layers, and gastrointestinal tracts such as the esophagus and intestine. Notably, intestinal sections consisted of 27–28 lining cells containing 0–4 nuclei per cell. We tentatively identified the nematode larva recovered from the vocal cord cystic lesion as the third-stage larva of Gnathostoma, probably G. nipponicum or G. hispidum, based on the sectional morphologies.
Introduction
Vocal cord cysts are less frequent than other types of vocal cord diseases, including vocal polyps, nodules, and Reinke’s edema. Vocal cord cysts change voice, such as diplophonia and voice limitation. An indirect laryngoscopic examination may misdiagnose a vocal cord cyst as a vocal cord polyp or nodule. Therefore, the laryngeal stroboscopic examination is crucial to diagnose a vocal cord cyst. Vocal cord cysts are commonly caused by vocal cord overusage or upper respiratory tract infections [1].
Gnathostoma spp. (Nematoda: Gnathostomatidae) are the parasitic agent of human gnathostomiasis. Among the 12 species in the genus, at least 5, including G. binucleatum, G. doloresi, G. hispidum, G. nipponicum, and G. spinigerum, cause human disease [2]. The first intermediate host is copepod, and the second hosts include fish, frogs, snakes, or poultry, of which raw or undercooked meat causes human infection. Definitive hosts are domestic or wild felines and canines for G. spinigerum, domestic or wild pigs for G. hispidum, and weasels for G. nipponicum [3]. Gnathostoma hispidum was recovered in Korea from an erythematous papule on the back of a 74-year-old man who returned to Korea in 2010 after living in China for 60 years [4]. An imported case of intraocular gnathostomiasis was reported in 2012 in a 15-year-old man returning from a trip to Vietnam after consuming raw wild boar meat and lobster [5]. However, the case was diagnosed by serologic testing, and the species could not be confirmed. One case of G. spinigerum infection in the upper lip was reported in a woman in 2013 who had not traveled abroad [6]. G. hispidum L3 larvae were recovered from a snake in 1998 [7]. G. nipponicum larva infections were confirmed in frogs and snakes on Jeju Island in 2011 [8]. Adult worm infections of G. nipponicum were found in a weasel on Jeju Island, indicating the existence of a domestic life cycle of G. nipponicum [9]. Vocal cord cyst originated from Gnathostoma spp. has not been traced in the literature databases including PubMed.
This case report presents gnathostomiasis found in a vocal cyst in a 54-year-old Chinese woman living in Korea who complained of voice changes. The patient provided informed consent to publish this case report. The case was described following the CARE statement (https://www.care-statement.org/). This report indicates that Gnathostoma infection should be considered in the differential diagnosis of vocal cord cysts.
Case Description
A 54-year-old Chinese housewife who lived in Anyang, Gyeonggi-do, Korea, visited the outpatient department of otorhinolaryngology at Hallym Sacred Heart Hospital, Hallym University, in Anyang, on August 2, 2021. She complained of the voice change that occurred 3 months ago. The patient reported eating raw conger a few weeks before the voice change developed. She had no digestive symptoms, such as abdominal pain and vomiting, or general symptoms, such as fever and chills. Her medical history revealed no specific disease.
Complete blood counts revealed a hemoglobin level of 11.7 g/dl, a white blood cell count of 3,100/mm3 (eosinophils 2.8%), and a red blood cell sedimentation rate of 11 mm/h. A rigid laryngoscopic examination revealed a round, red cystic lesion measuring approximately 4 mm in diameter was observed in the anterior part of the right vocal cord (Fig. 1).
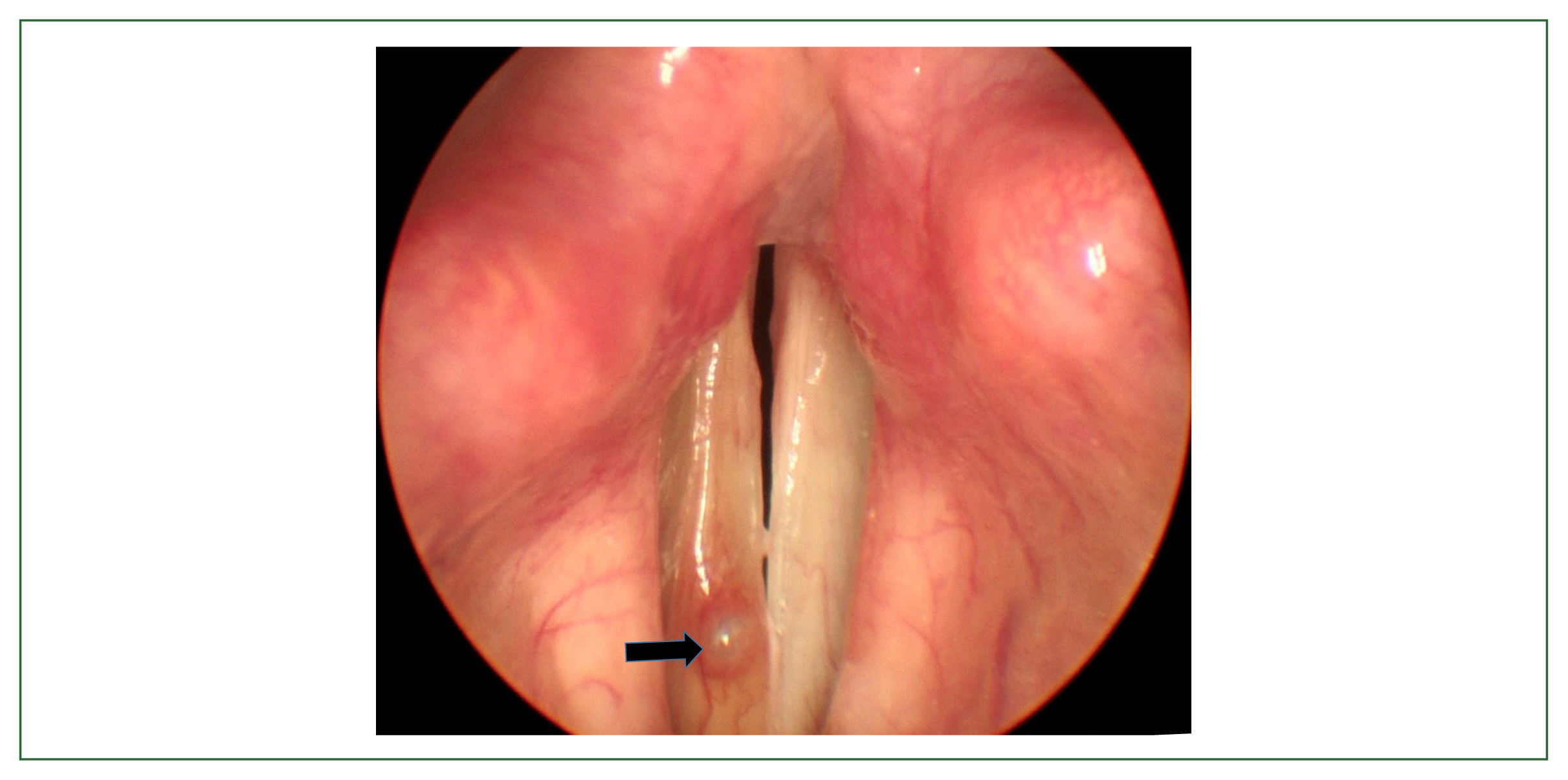
A cyst in the right vocal cord (arrow) of a 54-year-old woman who complained of voice change lasting for 3 months.
The cyst was removed using forceps and scissors through laryngeal microsurgery under general anesthesia, and the surgery was terminated without any specific issue. The cystic lesion and vocal cord tissues, identified under a microscope during surgery, demonstrated no visible parasites or larvae. However, the final histopathological examination of the cyst identified an inflamed region of soft tissue, including the worm.
The cyst wall was composed of inflammatory cells and fibrotic tissues (Fig. 1). Three sections of larva were discovered in the cyst at the esophagus level and the beginning of the intestine. The worm sections varied in diameter, from 190 μm to 235 μm. More intensely stained tegumental spines are observed in the outer cuticular layer. Polymyarian–coelomyarian somatic muscle layers were observed under the cuticle. The section of the upper left position is the longitudinal section of the esophageal level. The other 2 sections are at the intestinal level. The intestinal canal consisted of 27–28 lining cells, each with 0–4 nuclei in the center. Lateral cords were found, but they are tiny (Figs. 2, 3). These findings identified the larva as an advanced third-stage G. nipponicum or G. hispididum [4]. G. nipponicum has more nuclei in the intestinal cells than G. hispididum to which our specimen well corresponded (0–4 nuclei). However, the body width is too large compared to that of G. nipponicum. The number of lining epithelial cells in our case, 27–28 cells, corresponds to G. hispidum. However, molecular genetic analysis using paraffin-mounted nematode tissue failed, making it difficult to confirm a definitive diagnosis.
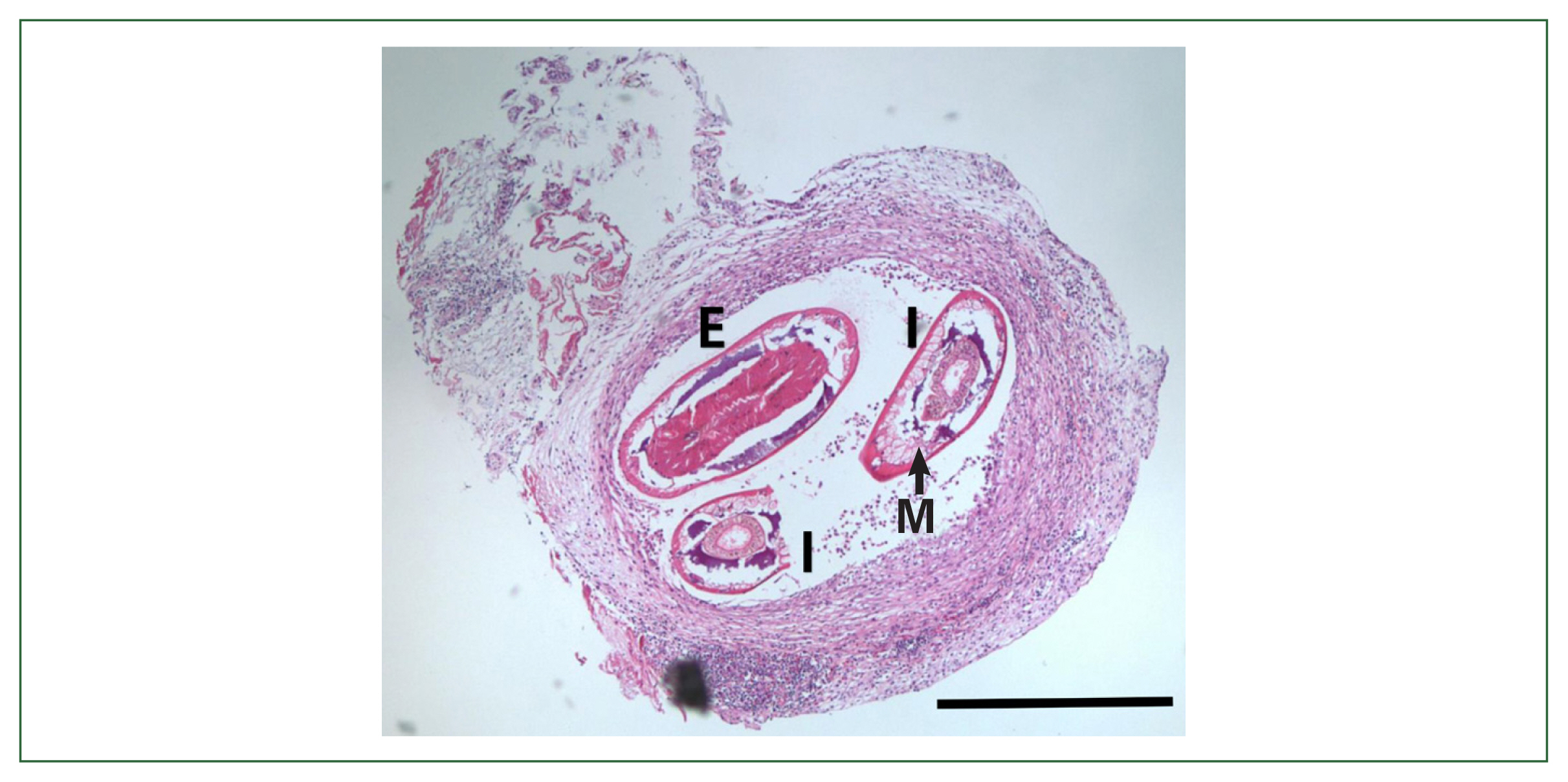
Histopathological examination of the cyst shows sections of the intestine and esophagus of Gnathostoma sp. Three larva sections were found in the cyst at the esophagus level and the beginning of the intestine. Polymyarian–coelomyarian somatic muscle layers (M) were seen under the cuticle. The section upper left position is the longitudinal section of the esophageal level (E). The other 2 sections are at the intestinal level (I). The diameters of worm sections differ from 190 μm to 235 μm. Bar=200 μm.
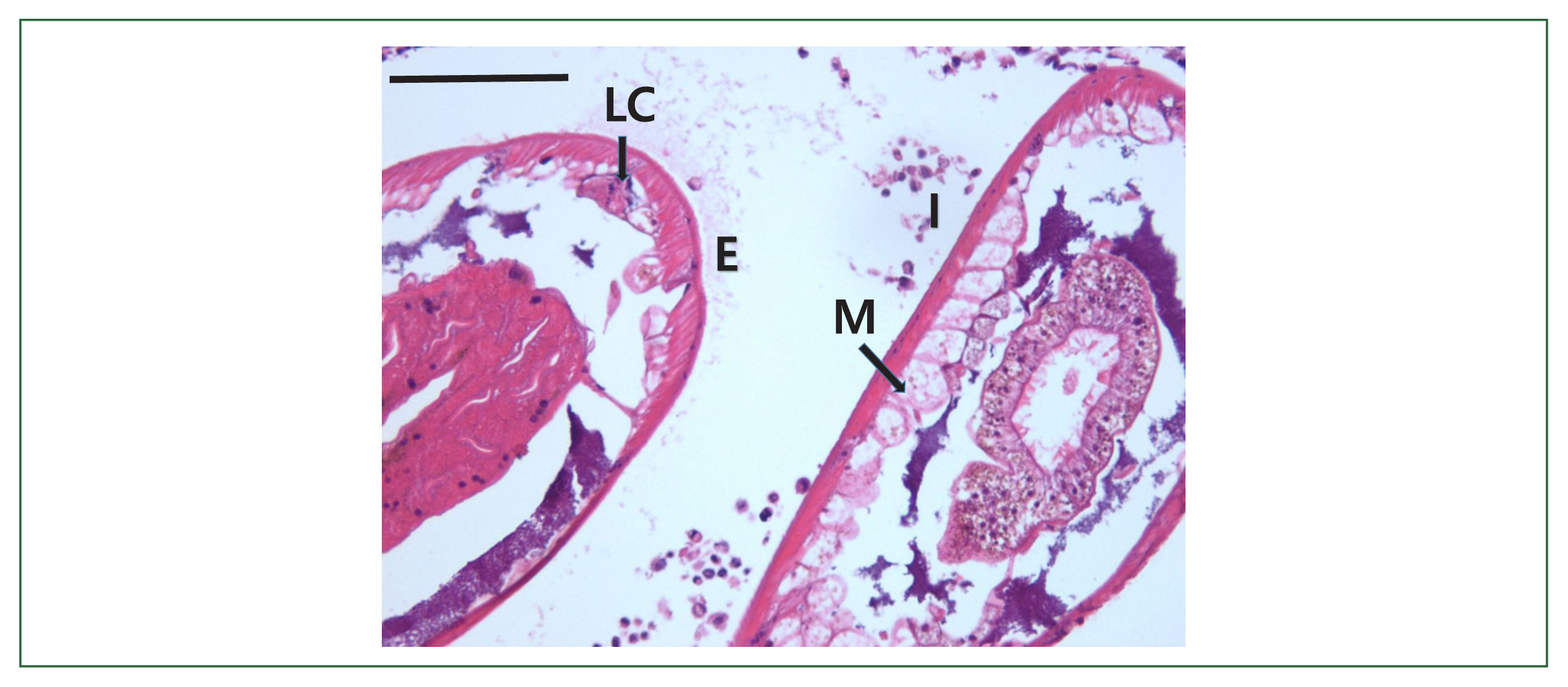
Histopathological examination of the cyst shows sections of the intestine and esophagus of Gnathostoma sp. for specific structure description. More intensely stained tegumental spines (arrows) are observed in the outer cuticular layer. Polymyarian–coelomyarian somatic muscle layers (M) were seen under the cuticle. The section upper left position is the longitudinal section of the esophageal level (E). The other 2 sections are at the intestinal level (I). The intestinal canal consisted of 27–28 lining cells, each with 1–4 nuclei in the center. Lateral cords (LC) were found, but they are tiny. Bar=50 μm.
The patient was referred to the gastroenterology department and underwent upper and lower gastrointestinal endoscopies, which revealed no specific findings. Her voice returned approximately 1 month after the cyst removal. The follow-up examination was terminated after 2 months because a flexible laryngoscope examination of the throat revealed no more specific findings (Fig. 4).
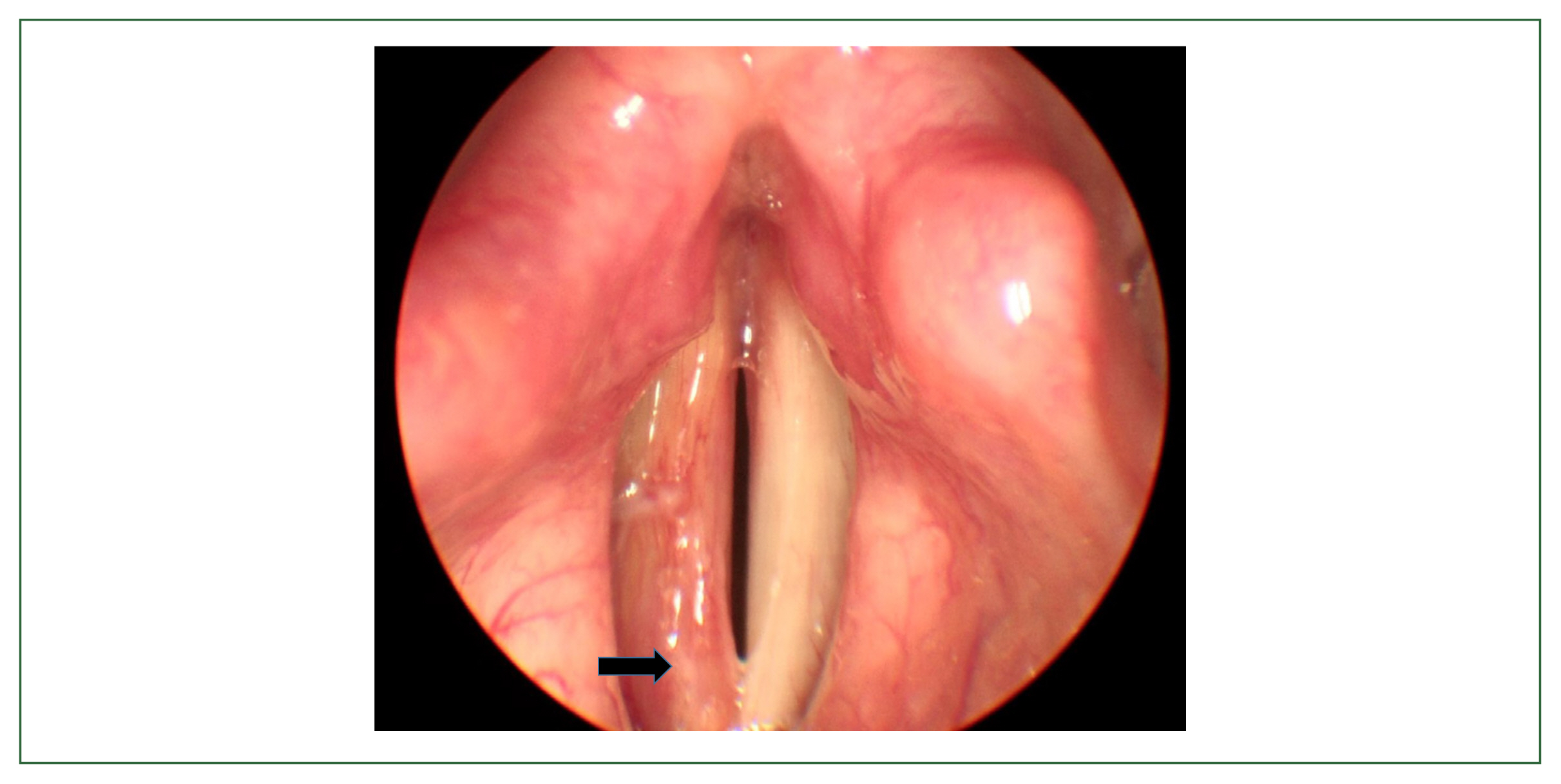
The vocal cord lesion is almost healed one month after resection. Arrow indicated the healed lesion.
Discussion
We demonstrated the progression of a chronic infection caused by G. nipponicum or G. hispidum larva penetrating the submucosal layer of the vocal cord and forming a cyst. Histological findings of chronic gnathostomiasis were shown following the degree of larval degeneration. Peripheral neutrophil infiltration and inflammatory reaction were observed in this case. Literature databases reported no previous vocal cord gnathostomiasis in any country. Suspecting or diagnosing vocal cord cysts caused by Gnathostoma spp. is difficult. The present case was diagnosed based on histopathological findings. G. nipponicum or G. hispidum was indicated as a causative pathogen.
Numerous G. nipponicum infections have been reported in Japan. Five confirmed human cases presenting creeping eruption and pruritus were observed between 1991 and 1992. The etiological agents responsible for these cases are the advanced third-stage larvae of G. nipponicum. The affected individuals reported consuming raw freshwater fish, such as sockeye salmon (Oncorhynchus nerka), carp (Cyprinus carpio), crucian carp (Carassius gibelio langsdorfi), and common ice fish (Salangichthys microdon), in the weeks preceding the symptom manifestation [10]. A 60-year-old female in Japan exhibiting creeping eruption was diagnosed with cutaneous gnathostomiasis attributed to G. nipponicum through genetic analysis in 2001. She had consumed raw largemouth bass 3 weeks before her hospital visit [11]. A case of cutaneous gnathostomiasis in a 21-year-old Japanese woman, who ingested raw icefish, was caused by G. nipponicum via genetic analysis in 2019 [12]. Human infections with G. hispidium were reported in Korea from a 74-year-old man who complained of an erythematous papule on his back [4]. Three cases were reported in Japan: a 55-year-old man who experienced stomach pain with a fever of 41°C and creeping eruption on his abdomen after eating a raw snake; a 25-year-old man who suffered from a fever of 39°C, pulmonary infiltration, and creeping eruption after eating raw loaches; a 44-year-old man who complained of linear erythema on his left trunk 2 months after eating raw loaches [13]. Third-stage larvae of G. nipponicum were detected in frogs and snakes on Jeju Island [8] and adults of G. nipponicum infection was identified in a weasel on Jeju Island [9], but no human infections by G. nipponicum had been reported in Korea. Therefore, the possibility of infection in Korea or China should be considered. Studies reported G. nipponicum infection in the intermediate hosts imported from China. Six early third-stage larvae of G. nipponicum were recovered from the muscle of 376 loaches (Misgurnus anguillicaudatus) imported from China in March 1992 [14]. The presence of the larval gnathostome was examined in 9,493 loaches imported from China from May 1993 to April 1994, of them, 369 (3.9%) demonstrated larvae of G. hispidium [15]. A total of 205 larval gnathostomes were collected from 18 (22.5%) of 80 red banded odd-tooth snakes (Dinodon rufozonatum rufozonatum), which had been smuggled from China and confiscated at Customs in Busan, Korea, in October 2002. The larvae were identified as the third-stage larvae of G. hispidum [16]. Infection is possible in Korea or China according to the presence of case reports and reports of intermediate hosts in both countries, as previously described.
This report had some limitations. Information about this patient’s medical history, including the date of entry and exit from Korea and food sources (fish, amphibians, and/or reptiles) in her hometown or residence in China, was lacking. The exact species identification was difficult according to the sectional morphology, including the number of intestinal cells and the number of nuclei in the intestinal cell. Molecular biological analysis using the paraffin-embedded sample was also unsuccessful. Therefore, the exact species could not be identified at this moment.
This case is an example of chronic gnathostomiasis that formed an inflammatory cyst after soft tissue invasion. This rare case indicates that gnathostomiasis should be considered as a cause of vocal cord cysts in regions where eating raw or undercooked fish, frogs, snakes, or poultry is common. Verifying the source of infection was impossible in this case because conger is not known as the second intermediate host of Gnathostoma spp. Whether the patient was infected in Korea or China remains unclear, but she may be infected in Korea because it is challenging for her to visit China before visiting the otorhinolaryngology department before August 2021 due to the coronavirus disease-2019 pandemic in Korea and China. Otorhinolaryngologists should consider gnathostomiasis as a cause of vocal cord cysts in the differential diagnoses before surgical removal in Gnathostoma spp. prevalent areas.
Acknowledgments
The species identification was indebted to Dr. Jong-Yil Chai, Professor Emeritus of Seoul National University College of Medicine, and Dr. Woon-Mok Sohn, Professor Emeritus of Gyeongsang National University College of Medicine.
Notes
Author contributions
Conceptualization: Park DS, Cho EH, Park KH, Jo SM, Park B, Huh S
Data curation: Park DS, Cho EH, Park KH, Jo SM, Park B
Methodology: Cho EH, Park KH, Huh S
Resources: Park DS, Cho EH, Park KH, Jo SM, Park B
Validation: Huh S
Visualization: Park KH, Jo SM, Park B
Writing – original draft: Park DS, Cho EH, Park KH, Jo SM, Park B, Huh S
Writing – review & editing: Park DS, Cho EH, Park KH, Jo SM, Park B, Huh S
The authors declare no competing interests.