Abstract
Cat flea bite in humans results in extremely pruritic skin lesions. It has been reported to occur among those living in domiciliary accommodation. However, nosocomial infestation with cat flea has not been reported. We hereby report a case of nosocomial infestation of cat flea in a hospital facility. Identification of the parasite, its appropriate eradication, and adequate medical management of the patients resulted in a satisfactory outcome.
-
Key words: Ctenocephalides felis, cat flea, nosocomial infection, Malaysia
INTRODUCTION
Cat and dog fleas are the most common parasites responsible for flea bite in humans. Cat flea bite results in extreme pruritis which may be prolonged if not identified early. It requires appropriate medical management and eradication of fleas from the environment to achieve treatment success. Cat flea infestation is commonly seen in pet day care or storage compounds. To our knowledge 2 cases of cat flea bites have been reported among medical students living in hostel facilities [
1,
2]. Although cat flea bite can occur in humans, many of the incidences are not brought to medical personnel's attention early, resulting in chronic skin discomfort. We report a rare case of nosocomial infestation with cat flea in a hospital in Malaysia. Due to its rare occurrence, we need to create awareness among physicians to consider this as differential working diagnosis in cases of skin rash outbreak in an institution.
CASE REPORT
Six nurses were referred for consultation in December 2010 after experiencing extreme pruritits of 2 months duration. On further enquiry, 3 other allied health personnel servicing the ward and 2 patients reported to have similar complaints. The staffs described pruritis as typically lasting for several days, worsening during working days and relieved during weekends and off days. Pruritis was experienced throughout the day and not associated with night time exaggeration. No other family members of the staffs were affected. Clinically multiple erythematous, urticated plaques of similar appearance (monomorphic), about 0.5 cm in diameter were noted mainly over the exposed areas of the ankles, neck, and abdomen (
Fig. 1). The genitalia was spared. Identical lesions were found on all those involved. All of them did not have any previous skin disorders except one who had childhood history of eczema. A diagnosis of papular urticaria with a differential diagnosis of papular eczema was made. Since all those affected had similar lesions and were stationed at the same location, the ward was visited for inspection.
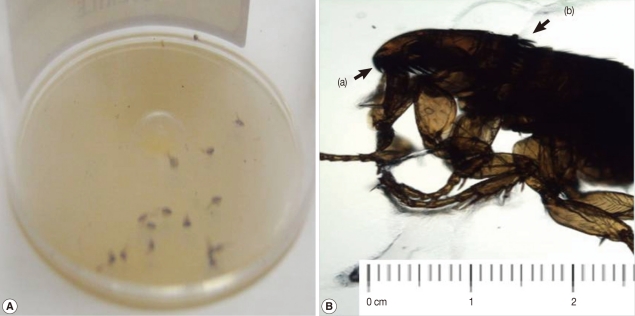
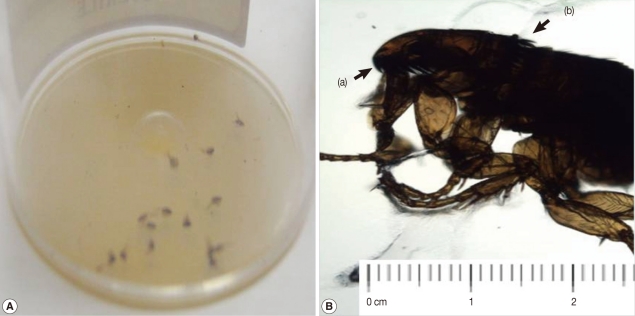
Multiple small black colored insects of less than 0.5 cm in size were found in the dirt swept from the floor of the ward (
Fig. 2A). These insects were then collected and sent to the parasitology unit for further inspection and analysis. Microscopic examinations revealed reddish brown wingless insects with multiple large spines on the head (=genal comb) and also on the thorax (=pronotal comb) (
Fig. 2B). Other features were the short bristle on the dorsal margin of the hind tibia and the anteriorly pointing elongated frons. These morphological features conformed to the description of cat flea,
Ctenocephalides felis as described by Iyengar et al. [
3].
This confirmed our clinical diagnosis of cat flea bite. All the patients and staffs who were affected were treated with topical steroid of moderate potency and oral anti-histamines for symptomatic relieve of pruritis for a total of 4 to 8 weeks. None of these patients developed any secondary eczematization or bacterial infection. Patients responded well and had complete resolution of the symptoms. The hospital infection control team was notified for further management of the infested ward. All patients and their belongings were shifted temporarily to a different ward before fumigation. Fumigation was done to the floor, walls, and furniture's of the ward using insecticide and insect growth regulators (IGRs) containing methoprene or pyriproxyfen. Fumigation was repeated after 2 weeks as the first process did not achieve total eradication. However, no stray cats were identified within the hospital premises.
DISCUSSION
Fleas are small parasitic wingless insects of the order Siphonaptera. The commonest flea species associated with humans is the cat flea (
Ctenocephalides felis) which is also the most important ectoparasite of domestic cats and dogs worldwide. These insects are tiny measuring about 1.5 to 4.0 mm in length and survive well in warm and humid temperature. Adult fleas are able to jump up to about 1 foot with the aid of their long legs. Their life expectancy is short, approximately 2-3 months. After mating, the female fleas lay eggs in the host's fur which dislodges on to the floor, carpets, dark dusty corners, cracks on the wall, or bedding. The eggs then hatch in these rest areas and progress in their stages into larvae, pupae, and adult fleas [
4]. The primary host for this insect is the cat. The blood of the cat is required for its reproduction process and it is unable to sustain its lifecycle in humans. Humans play the role of a temporary host in providing a blood meal; however, it is able to survive in the absence of a host for many months. Only about 1-5% of the flea population live on their hosts, while the remainder spread around the habitat, e.g., the animal resting or feeding areas [
5]. Beck et al. [
5] reported that male cats appeared to have a remarkably higher rate of flea infestations compared to female cats.
Fleas are notorious human pathogens due to their bites which resulted in significant cutaneous discomfort and potential secondary cutaneous infections. The commonest cutaneous manifestation is papular urticaria, which is an allergic reaction leading to intense pruritus which may last for several weeks as described in this case. All those who are exposed to it are affected as has been reported among students staying in institutions by Chin et al. [
1] and Noor Hayati et al. [
2]. Nevertheless, not all individuals experience similar symptoms as some may become desensitized and not experience any itchiness. Besides causing allergic reactions, members of some species of fleas may potentially act as vectors and transmit disease organisms, such as bubonic plague and murine typhus. One study has reported the possibility of murine typhus infection and cat flea rickettsiosis in humans resulting from cat flea bite [
6]. Sources of cat fleas in this hospital infestation may arise from stray cats hiding in secluded areas of the hospital, such as the space underneath the staircase or in the vicinity of the kitchen and cafeteria. Adult fleas can be transported to the ward by hitching a ride on human clothes facilitating movement in and out of wards. In addition, the adult fleas may also be carried out by staffs or visitors from their home to the work place.
The infection control team needs to be alerted to manage the infested ward as its eradication requires fumigation with insecticides. Regular vacuuming of corners, indoor, and outdoor aerosol spray with IGRs containing methoprene or pyriproxyfen is beneficial in eradicating the cat flea in all stages of its lifecycle [
7]. Another agent which was shown to be effective is selamectin spot-on formulations applied to cats against adult cat fleas, flea eggs, and adult flea emergence. Dryden et al. [
8] reported significant reduction in egg production and larval and adult emergence during the entire 6 weeks of therapy with either selamectin or fipronil-(S)-methoprene [
8]. Topical pyriprole solution is also efficacious due to its ability to disrupt the flea life cycle by killing adult fleas before they lay eggs. This disruption extends up to 30 days after treatment initiation [
9].
Hot water wash is advised for treating linen and patient's clothing to eradicate the eggs, larvae, and pupa [
10]. Besides that, hospital premise, such as cafeterias, kitchens, and vents should be regularly monitored and cleared of any furry animals as these places provide comfortable home for stray animals. It is hoped that this case report will increase awareness among physicians and the hospital infectious control staff that parasites are capable of causing nosocomial infection, and the knowledge of both patient treatment and parasite eradication is important.
References
- 1. Chin HC, Ahmad NW, Lim LH, Jeffery J, Hadi AA, Othman H, Omar B. Infestation with cat flea, Ctenocephalides felis (Siphonaptera: Pulicidae) among students in Kuala Lumpur, Malaysia. Southeast Asian J Trop Med Public Health 2010;41:1331-1334.
- 2. Noor Hayati MI, Jeffery J, Anisah N, Yusof S. Maculopapular rashes caused by cat flea, Ctenocephalides felis (Siphonaptera: Pulicidae) bites in a university student. Trop Biomed 2002;19:131-134.
- 3. Iyengar R. The Siphonaptera of the Indian subregion. Oriental Insects 1973;15-19.
- 4. Milne L, Milne M. National Audubon Society Field Guide to North American Insects and Spiders. 1996. New York, USA. Alfred A. Knopf.
- 5. Beck W, Stickel M. Interhost migration behavior of Ctenocephalides felis on cats and in their resting sites. Wien Klin Wochenschr 2008;120:40-44.
- 6. Goddrard J. Fleas and human disease. Infect Med 2005;22:402-405.
- 7. Blagburn BL, Dryden MW. Biology, treatment, and control of flea and tick infestations. Vet Clin North Am Small Anim Pract 2009;39:1173-1200.
- 8. Dryden M, Payne P, Smith V. Efficacy of selamectin and fipronil-(S)-methoprene spot-on formulations applied to cats against adult cat flea (Ctenocephalides felis), flea eggs, and adult flea emergence. Vet Ther 2007;8:255-262.
- 9. Barnett S, Luempert L, Schuele G, Quezada A, Strehlau G, Doherty P. Efficacy of pyriprole topical solution against the cat flea, Ctenocephalides felis, on dogs. Vet Ther 2008;9:4-14.
- 10. Wilson J. Infection control in clinical practice. 2006. 3rd ed. New York, USA. Bailliere Tindall/Elsevier.
Fig. 1Multiple erythematous urticated plaques (arrows) on the abdomen (A) and the upper part of back and neck (B).

Fig. 2Small black-colored insects, i.e., cat fleas (A), and a miscroscopic view of a flea, Ctenocephalides felis (B), showing its genal (a) and pronotal combs (b).
Citations
Citations to this article as recorded by

- A One Health Perspective on the Resurgence of Flea-Borne Typhus in Texas in the 21st Century: Part 1: The Bacteria, the Cat Flea, Urbanization, and Climate Change
Gregory M. Anstead
Pathogens.2025; 14(2): 154. CrossRef - The First Report on Cat Flea (Ctenocephalides felis), a Zoonotic Haematophagous Insect Infestation in Humans in Bangladesh: A Case Report and Literature Review
Nusrat Nowrin Shohana, Md. Shahadat Hossain, Sharmin Shahid Labony, Md. Haydar Ali, Md. Abdul Alim, Ashim Kumar Nandi, Anisuzzaman
Veterinary Medicine and Science.2025;[Epub] CrossRef - Why do cat flea infestations often occur on the upper limbs and trunk? Fleas do not fly…
Stefano Veraldi, Rossana Schianchi, Gianluca Nazzaro, Italo Francesco Aromolo
Dermatology Reports.2025;[Epub] CrossRef - New insights into the haplotype diversity of the cosmopolitan cat flea Ctenocephalides felis (Siphonaptera: Pulicidae)
Noor Azrizal-Wahid, Mohd Sofian-Azirun, Van Lun Low
Veterinary Parasitology.2020; 281: 109102. CrossRef - The Biology and Ecology of Cat Fleas and Advancements in Their Pest Management: A Review
Michael Rust
Insects.2017; 8(4): 118. CrossRef