Abstract
We present here a 44-year-old male patient with hydatid disease who was referred to our hospital due to dyspnea and chest pain for the last 2 month before admission. Using echocardiography and contrast-enhanced computed tomography the heart hydatid was diagnosed. However, hydatid disease of the interventricular septum is rare; particularly, the involvement of mitral apparatus with mitral regurgitation (MR) is an exceptionally rare presentation. Early diagnosis and an integrated treatment strategy are crucial. Surgical excision was performed and the patient had an uneventful recovery and follow-up at 3 months.
-
Key words: Echinococcus sp., hydatid cyst, interventricular septum, papillary muscle
INTRODUCTION
Hydatidosis is a common disease in Iran [
1]. In the typical cycle,
Echinococcus tapeworm eggs are passed in the feces of an infected carnivorous animal and may subsequently be ingested by humans; they hatch into embryos in the intestine, penetrate the intestinal lining, and carried by blood throughout the body to major organs such as the liver, lungs, and heart. After the growing larvae localize in an organ, they transform into echinococcal cysts in which numerous tiny protoscolices are produced via asexual reproduction [
2]. In most patients, the cysts calcify and become asymptomatic.
Potentially it may cause right or left ventricular outflow obstruction, tricuspid regurgitation, aortic stenosis, myocardial dysfunction, conduction disturbances, stroke, or may lead to congestive heart failure. Cardiac hydatid cysts are rare among the cases of hydatid disease. The most frequent location in the heart is left ventricular free wall and the interventricular septum [
3-
5]. Clinical presentation of cardiac echinococcal cysts depends on the site, size, calcification, and number of cysts, integrity of the cyst, and presence of complications as the result of cyst rupture [
6,
7]. Dibello and Menenotez [
8] reported that a cyst rupture into the pericardium may cause acute pericardial tamponade, secondary pericardial cysts, or constructive pericarditis. Madariaga et al. [
9] showed that the rupture of subendocardial cysts, which otherwise may be silent, may cause anaphylactic shock and sudden death, peripheral and cerebral embolism, or pulmonary embolism. Agarwal et al. [
10] reported that intracavitary expansion and rupture of the cyst caused dyspnea or right outflow obstruction, pulmonary embolization, pulmonary hypertension, and death.
Ameli [
11] and Dibello [
8] reported that acute coronary syndrome secondary to the compression or emboli to the coronary artery may mimic coronary artery disease. According to Dighiero et al. [
12], the resulting pain of pericarditis may radiate to the epigastrium and, it may closely mimic acute abdomen. Uysalel et al. [
13] reported that a case of myocardial hydatid cyst mimicked left ventricular aneurysm. Other complications included mitral regurgitation (MR), papillary muscle ischemia, atrioventricular conduction defects. Arrhythmia was also report in a study by Agarwal et al. [
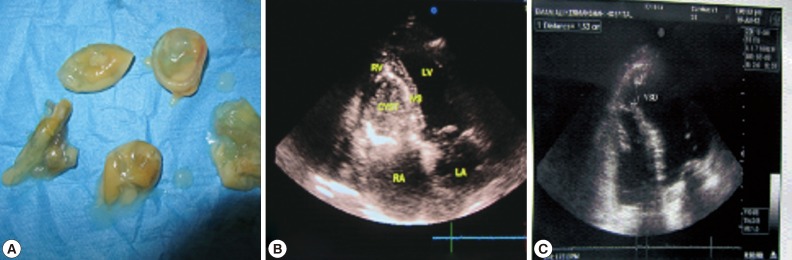
10]. In the present study, we encountered a 44-year-old male patient with hydatid disease in the intraventricular septum of the heart with papillary muscle involvement and clinical symptoms of dyspnea and chest pain. The preoperative diagnosis was established using echocardiography and confirmed after recovery of hydatid daughter cysts (
Fig. 1A).
CASE RECORD
A 46-year-old man non-smoker was admitted to our hospital due to dyspnea and chest pain for the last 4 months that exacerbated some days before admission. He did not complain of any other symptoms. He gave exposure to dogs and having reared sheep. The physical examination revealed no specific findings except precordial systolic souffle. Lung auscultation revealed a normal intensity of breath sounds. Electrocardiogram (ECG) did not show any remarkable findings except for right bundle branch block (RBBB). All routine laboratory test results, including liver and kidney function tests, serum proteins, and urine analysis were normal. The erythrocyte sedimentation rate was abnormal (ESR 60 mm/hr). Serology for echinococcosis showed an indirect immunohemagglutination test positive. Chest x-ray was normal. The computed tomography (CT) scan of the abdomen and thorax showed no disease. Transthoracic contrast echocardiography revealed a huge cyst like a hypodense structure (65×55 mm), located in the interventricular septum and the base of papillary muscle with distortion of mitral wall apparatus (i.e., papillary muscles) and moderate MR (
Fig. 1B). The rest of examination was normal with an estimated ejection fraction of 45%, without regional wall motion abnormalities. Coronary angiography revealed normal coronary arteries.
The patient underwent median sternotomy, and excision of the cardiac cyst was planned by using cardiopulmonary bypass. The patient received albendazole preoperatively with the dose of 800 mg daily for 2 weeks. After a median sternotomy, the patient was connected to the cardiopulmonary bypass by cannulating the ascending aorta and superior and inferior vena cava. There was no sign of pericarditis, and pericardial cavity was free of fibrosis and adhesions. Under a condition of hypothermic cardiopulmonary bypass, the aorta was cross-clamped and the heart was arrested with a dose of antegrade cold cardioplegia. The right atrium was opened that revealed bulging of the septum that was calcified as a white and hard mass in the right ventricular aspect of the septum (
Fig. 1C). The pericardial cavity was localized by pad moistened by ethanol 96%, and 10 ml ethanol was injected to the cyst cavity and after 5 min non-viscous yellow painted fluid was aspirated. A large incision was made into the right ventricular aspect of the septum corresponding to cyst's free wall.
The sub-septal wall of the cyst was calcified, fibrotic, and was not excised but its contents included the glistening germinative layer and daughter cysts were sucked out (
Fig. 1A), which were sent to histopathological examinations (
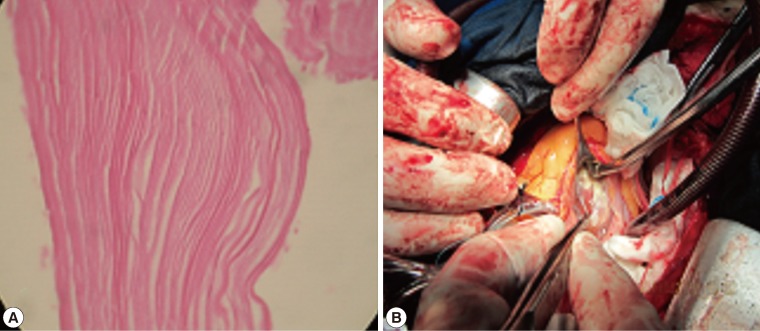
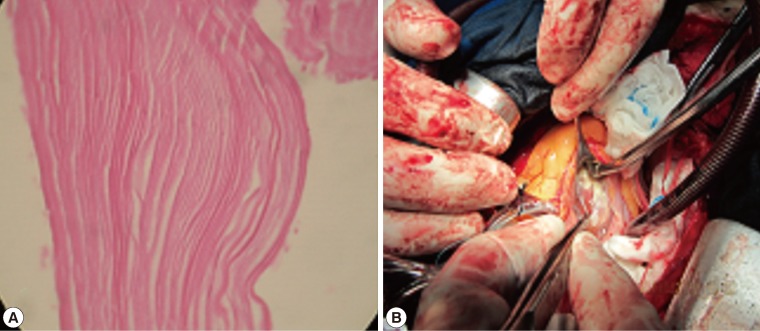
Fig. 2A). The cyst was then washed with 5 ml of povidone iodine solution, which was left inside for 5 min and then aspirated. The resultant cavity made by intraseptal partitioning was then obliterated by approximation of its fibrosis walls with 4-0 viline suture to complete this obliteration. We explored the left ventricle via the left atrium that revealed involvement of the base of huge anterior papillary muscle as a subsidiary horn. The muscle was opened at its medial aspect in conjunction with the septum. The residual hydatid cyst, which contained membranes and daughter vesicles, was removed. The remaining cavity was left open. The septal involvement by the cyst caused distortion of the mitral apparatus by papillary muscle elongation. Anterior mitral leaflet prolapse that has normal segment of the P1 and P2 scallops were repaired by means of corda tendina shortening.
Pathological examinations of the daughter cyst and fluid revealed germinative layers (
Fig. 2A). Normalized lengthening of the papillary muscle and corda tendina eliminated moderate MR post-operatively. After operation, transesophageal echocardiography revealed a venticule septal defect (VSD) in the base of the anterior papillary muscle which was repaired with 4-0 viline sutures (
Fig. 2B). The patient had an uneventful recovery and at the 7th postoperative day she was discharged from the hospital with an acceptable echocardiography findings which revealed near normal functions of the mitral valve apparatus, with only mild regurgitation.
DISCUSSION
Involvement of the heart by hydatid cysts can occur through the inferior vena cava to the right atrium and directly to the right atrial wall or trans-septaly through the interatrial septum to the left atrium or trans-septaly to the left ventricle or remains intra-septaly. Another way is through the pulmonary artery to the lung and from the pulmonary vein to the systemic circulation or intra-heart cavity to any part of the heart structure like atria and ventricles but involvement of papillary muscles concomitantly with interventricular septum and MR is exceptionally rare and careful literature evaluation revealed only a few cases [
14]. Birincioglu et al. [
15] revealed that the prevalence of left and right atrium is 4% of heart structure involvement. Intracavitary cyst rupture is the most dangerous sequele of heart echinococcosis. Odev et al. [
16] and Lahdhili et al. [
17] documented that, due to the effect of pump, the left ventricle cysts perforated in the aorta but the right ventricle cysts perforated intracavitary. Unlu et al. [
18] and Kopp et al. [
19] showed that the incidence of intracardiac perforation is between 20-40% and after a cyst perforation 75% of the patients died from septic shock or embolic complications.
Heart is only organ that can be treated by surgery; however, other organs may be treated both by chemotherapy and surgical manipulations. In the case of heart echinococcosis it is impossible to administer anthelmintic medications prior to a surgery due to the risk of cyst wall destruction and rupture. In addition, the results of surgical treatment of heart echinococcosis are better than those treated by the conservative strategy only [
20]. The present unusual and exceedingly rare case exemplifies that one has to keep the hydatid cyst in the differential diagnosis of a mixed echogenic mass in the interventricular septum on echocardiography that complicated preoperatively by MR and post-operatively by VSD.
In view of the rarity of combined the septal and papillary muscle involvement by the hydatid cyst that complicated by pre-operative MR, surgical treatment of cardiac echinococcosis is emergent. In conclusion, the treatment of heart echinococcosis should be a combination of surgical intervention with chemotherapy during or post-operative period aiming to decrease the recurrences.
References
- 1. Sadjjadi SM. Present situation of echinococcosis in the Middle East and Arabic North Africa. Parasitol Int 2006;55:S197-S202.
- 2. Rostami Nejad M, Nazemalhosseini Mojarad E, Norouzina M, Fasihi Harandi M. Echinococcosis: based on molecular studies in Iran. Gastroenterol Hepatol From Bed to Bench 2010;3:169-176.
- 3. Battelli G, Mantovani A, Seimenis A. Cystic echinococcosis and the Mediterranean region. Parassitologia 2002;44:43-57.
- 4. Long WJ. Hydatid disease in left ventricular wall of the heart. Med J Aust 1932;2:701.
- 5. Al-Naaman YD, Samarrai AA, Al-Omeri MM. Hydatid disease of the heart. A report of four cases. J Cardiovasc Surg (Torino) 1973;14:95-101.
- 6. Sinha PR, Jaipuria N, Avasthey P. Intracardiac hydatid cyst and sudden death in a child. Int J Cardiol 1995;51:293-295.
- 7. Perez-Gomez F, Duran H, Tamames S, Perrote JL, Blanes A. Cardiac echinococcosis: clinical picture and complications. Br Heart J 1973;35:1326-1331.
- 8. Di Bello R, Menenotez H. Intracardiac rupture of hydatid cysts of heart. A study based on three personal observations and 101 cases in the world literature. Circulation 1963;27:366-374.
- 9. Madariaga I, De la Fuente A, Lezaun R, Imizcoz MA, Carmona JR, Urquia M, de los Arcos E. Cardiac echinococcosis and systemic embolism. Report of a case. Thorac Cardiovasc Surg 1984;32:57-59.
- 10. Agarwal DK, Agarwal R, Barthwal SP. Interventricular septal hydatid cyst presenting as complete heart block. Heart 1996;75:266.
- 11. Ameli M, Mobarhan HA, Nouraii SS. Surgical treatment of hydatid cysts of the heart: report of six cases. J Thorac Cardiovasc Surg 1989;98:892-901.
- 12. Dighiero J, Canabal EJ, Aguirre CV, Hazan J, Horjales JO. Echinococcus disease of the heart. Circulation 1958;17:127-132.
- 13. Uysalel A, Aral A, Atalay S, Akalin H. Cardiac echinococcosis with multivesicular involvement. Pediatr Cardiol 1996;17:268-270.
- 14. Ozer N, Aytemir K, Kuru G, Atalar E, Ozer Y, Ovunc K, Aksoyek S, Gokoz A, Gursel G, Kes S. Hydatid cyst of the heart as a rare cause of embolization: report of 5 cases and review of published reports. J Am Soc Echocardiogr 2001;14:299-302.
- 15. Birincioglu CL, Bardakci H, Kucuker SA, Ulus AT, Arda K, Yamak B, Tasdemir O. A clinical dilemma: cardiac and pericardiac echinococcosis. Ann Thorac Surg 1999;68:1290-1294.
- 16. Odev K, Acikgozoglu S, Gormus N, Aribas OK, Kiresi DA, Solak H. Pulmonary embolism due to cardiac hydatid disease: imaging findings of unusual complication of hydatid cyst. Eur Radiol 2002;12:627-633.
- 17. Lahdhili H, Hachicha S, Ziadi M, Thameur H. Acute pulmonary embolism due to the rupture of a right ventricle hydatic cyst. Eur J Cardiothorac Surg 2002;22:462-464.
- 18. Unlu Y, Ceviz M, Karaoglanoglu N, Becit N, Kocak H. Arterial embolism caused by a ruptured hydatid cyst in the heart. Surg Today 2002;32:989-991.
- 19. Kopp CW, Binder T, Grimm M, Merl O, Thalhammer F, Ullrich R, Heinz G, Mundigler G, Stefenelli T, Maurer G, Baumgartner H, Zehetgruber M. Images in cardiovascular medicine. Left ventricular echinococcosis with peripheral embolization. Circulation 2002;106:1741-1742.
- 20. Shevchenko YL, Travin NO, Musaev GH, Morozov AV. Heart echinococcosis: current problems and surgical treatment. MMCTS 2006;doi: 10.1510/mmcts.2005.001115
Fig. 1(A) Macroscopic view of the daughter cysts (each cyst 1 cm in length) (B) 4-chamber echocardiographic view of the hydatid cyst at the interventricular septum of the heart. (C) An intraoperative echocardiographic view of septal bulging of the hydatid cyst.
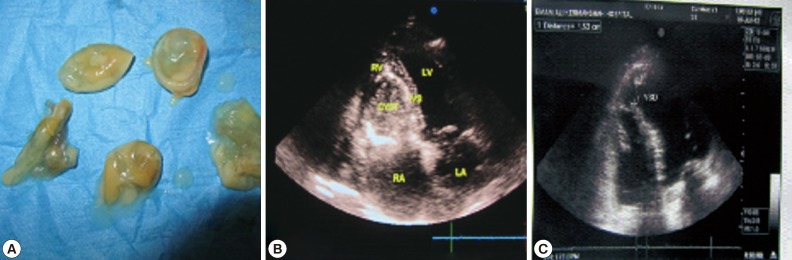
Fig. 2(A) Histological figure of the daughter cyst wall showing the presence of an inner germinal layer (×100). (B) A short-axis veiw depicting the clear boarders of iatrogenic post-operative ventricular septal defect.
Citations
Citations to this article as recorded by

- A cardiac hydatid cyst mimicking a pericardial tumour in a paediatric case
Taliha Oner, Oktay Korun, Ahmet Celebi
Cardiology in the Young.2019; 29(2): 244. CrossRef - Cardiac hydatid cyst in the interventricular septum: A literature review
S. Fennira, S. Kamoun, B. Besbes, I. Ben Mrad, I. Zairi, F. Ben Moussa, K. Mzoughi, S. Kraiem
International Journal of Infectious Diseases.2019; 88: 120. CrossRef - eComment. New horizons in diagnosing and managing cardiac echinococcosis
Tomislav Mestrovic, Mario Sviben
Interactive CardioVascular and Thoracic Surgery.2018; 26(2): 359. CrossRef - Analysis of Lethality in Echinococcal Disease
Anna S. Khachatryan
The Korean Journal of Parasitology.2017; 55(5): 549. CrossRef - Prevalence of Hydatid Cyst in Slaughtered Livestock in Kermanshah (West Iran)
Reza Faraji, Gholam Reza Javadi, Parisa Mohamadi Barshahi, Fereshte Ahmadian, Mohammadtaghi Sarebanhassanabadi, Ali Dehghani Firoozabadi, Abdol Rasoul Moloudi
Advances in Microbiology.2015; 05(04): 252. CrossRef - eComment. Evidence-based diagnosis and treatment of intraaortic cystic echinococcosis
Tomislav Mestrovic, Mario Sviben
Interactive CardioVascular and Thoracic Surgery.2015; 21(4): 549. CrossRef