Abstract
Echinococcus granulosus, an intestinal tapeworm of dogs and other canids, infects humans in its larval stage and causes human echinococcosis or hydatid disease. In the Republic of Korea, 31 parasite-proven human echinococcosis cases have been reported, most of which were imported from the Middle East. We recently examined a 61-year-old Korean man who had a large cystic mass in his liver. ELISA was negative for tissue parasitic infections, including echinococcosis, cysticercosis, paragonimiasis, and sparganosis. The patient underwent surgery to remove the cyst, and the resected cyst was processed histopathologically for microscopic examinations. In sectioned cyst tissue, necrotizing protoscolices with disintegrated hooklets of E. granulosus were found. In some areas, only freed, fragmented hooklets were detected. The patient had traveled to western and central Europe in 1996, and had no other history of overseas travel. We report our patient as a hepatic echinococcosis case which was probably imported from Europe.
-
Key words: Echinococcus granulosus, liver, case report, ELISA, histopathology, protoscolex
INTRODUCTION
Human echinococcosis or hydatidosis is a zoonotic disease caused by infection with the metacestode of
Echinococcus granulosus or
Echinococcus multilocularis, an intestinal tapeworm of the dogs, cats, and foxes [
1]. A wide range of mammals, including cattle, sheep, goats, marsupials, and primates, serve as intermediate hosts. In these animals,
E. granulosus causes cystic echinococcosis (CE) presenting with a large, unilocular cyst, whereas
E. multilocularis causes alveolar echinococcosis (AE) presenting with small, multilocular cysts. Humans are aberrant (accidental) hosts, and the parasite does not complete development into adults in human hosts [
1]. Endemic areas include the Mediterranean regions, the Middle East, the Russian Federation, the People's Republic of China, eastern and northern Africa, Australia, South America, and some European countries [
1].
In the Republic of Korea, a total of 31 echinococcosis cases have been reported in the literature based on identification of the parasite; the patients included 24 Koreans, 6 Uzbeks, and 1 Mongolian [
2-
16]. One recurring case in the peritoneal cavity was described in a Korean [
17]. Most of the cases were imported, with the exception of 2 Korean cases in which the origin of infection was obscure [
9,
18]. The remaining 22 Korean patients had a history of travel to or residence in highly endemic areas, including the Middle East (17 cases), Libya (1 case), Pakistan (1 case), Vietnam (1 case), China (1 case), and Brazil (1 case) [
2-
16]. We report here a presumed imported case of cystic echinococcosis (CE) in the liver of an otherwise healthy, 61-year-old man who had a travel history to western and central Europe.
CASE DESCRIPTION
In November 2008, a 61-year-old Korean man was transferred to the Seoul National University Hospital, Seoul, Republic of Korea for a large cystic liver mass detected by ultrasonography on health checkup. He did not have liver disease or any other medical problems. He traveled to Europe (France, German, Italy, Switzerland, and Spain) in 1996.
At ultrasonography, a heterogeneous echoic mass of about 8 cmin diameter was detected, and the characteristic 'ball of wool' appearance was recognized (
Fig. 1). In magnetic resonance imaging (MRI), the mass was characterized by a T1 low and T2 heterogeneous high signal intensity without enhancement. The tentative radiologic diagnosis was either of an atypical epidermoid cyst, a cystic teratoma, a pseudocyst, a foreign body reaction, or a parasite infection. The results of routine blood biochemistry were normal. Serological tests by ELISA to detect antibodies against
Taenia solium metacestode,
Paragonimus westermani, sparganum,
Clonorchis sinensis, and hydatid cyst (
E. granulosus) were performed. However, ELISA was negative for all the parasites. Regardless of this uncertain clinical setting, he received a tumorectomy because a slowly-growing large mass by itself is an indication for a surgical intervention.
In the Department of Pathology, the resected specimen was processed in a general manner. In gross examinations, the mass measured 9 × 6 × 5 cm (
Fig. 2). The cyst was filled with yellowish, necrotic liquid materials, and there was no solid mass growth inside the cyst (
Fig. 3). No grossly recognizable parasites or parasite eggs were detected in the necrotic materials under a stereomicroscope. However, small, spherical particles were identified that were not transparent enough to examine stereoscopically (photograph not taken). These particles were later identified as necrotizing protoscolices of
E. granulosus in light microscopic examinations of the sectioned histopathological specimens.
After fixation in 10% neutral buffered formalin, the cystic mass was sampled at several places according to standard procedures. The tissue samples were processed for serial, 3-µm thick paraffin sections and stained with hematoxylin and eosin (H-E) for conventional histopathological examinations. The liver parenchyma around the cyst showed signs of chronic granulomatous inflammation. The cyst was composed of a thick fibrous wall without lining epithelia and of extensive necrotic materials inside. Among the necrotic materials, many small structures resembling parasites and parasite eggs (
Figs. 4,
5) were recognized. Under the suspicion of a parasitic infection, the specimen was submitted to the Department of Parasitology and Tropical Medicine for further examination. Finally, the structures were identified as protoscolices and hooklets of
E. granulosus (
Figs. 4-
7), and the cyst wall was typically composed of a thick laminated layer (
Fig. 6). Thus, the cyst was confirmed to be a unilocular echinococcal cyst. Many of the protoscolices were necrotic and had lost their normal contour (
Fig. 6), but some had retained their suckers (
Fig. 4) or hooklets (
Fig. 5). There were also numerous freed hooklets (
Fig. 7), about 20 µm in length, embedded in the necrotic materials.
After the diagnosis, the ultrasonographic images were reviewed. According to the classification proposed by the WHO Informal Working Group on Echinococcosis [
1], the cyst was classified as an echinococcal cyst type CE 4 (medium size; 5-10 cm), which is inactive, with heterogenous degenerative contents (hyperechoic or hypoechoic), and without daughter cysts. Moreover, as the surgery was performed without any complications, no additional chemotherapy was needed. After the surgery, the patient did not show any sign of relapse.
DISCUSSION
The diagnosis of human echinococcosis is difficult even in large hospitals in the Republic of Korea, because this zoonotic disease is exotic and uncommon. In acute and active stages, radiological and serological tests, including ELISA, are useful for diagnosis [
1,
19]. However, in chronic and inactive stages, radiological examinations may reveal non-specific findings and serological tests may not be sensitive enough [
1]. Therefore, careful histological examinations are essential to diagnose chronic and inactive echinococcal cysts. In our case, the diagnosis could not be made until the surgically removed mass was processed for histopathological examination and light microscopy. The cyst was filled with necrotic materials, and degenerating protoscolices and hooklets of
E. granulosus were detected among these materials.
ELISA is a highly sensitive and useful serological test for echinococcosis, especially in its active stages. However, like other serological tests, ELISA may produce false negative results [
1]. False negatives may be due to the small size of a cyst (< 10 mm in diameter) and/or to the separation of the cyst from the surrounding tissue [
1]. In both cases, the concentration of parasite antigen may be too low to elicit humoral immune responses [
19].
In Korea, indigenous (presumed to be)
E. granulosus was reported in 1937 and 1944 with echinococcal cysts detected in cattle and pigs [
20,
21]. Around that time, the average prevalence in cattle was 0.73% nationwide (excluding Jeju-do Island) [
21]. On Jeju-do, the prevalence was much higher in bovines (6.8-27.5%) [
21]. This high prevalence in bovines on Jeju-do persisted until the 1970s [
20]. However, no further reports on bovine or swine echinococcosis were published after 1975 [
20]. Adult worm infection in dogs or other canids have never been reported in Korea. With regard to human echinococosis, 3 cases (2 were Koreans) were mentioned by H. Kobayashi in 1928, although they were not based on parasitological examinations [
18,
21].
Among the 31 parasitologically-proven echinococcosis cases reported in the Republic of Korea (1983-2009) (
Table 1), 24 were native Koreans between the ages of 25 and 66 years (mean: 40.9). Of these 24 cases, 21 (87.5%) were men. The organs involved were predominantly the liver (19 cases), followed by the lung (10 cases). The longest recorded incubation period was 33 years. With the exception of 2 Korean patients in whom the origin of infection is obscure [
9,
18], the remaining 29 cases are regarded as imported echinococcosis. The areas of acquisition were primarily the Middle East, and there were no cases imported from Europe. We consider that our patient is an echinococcosis case imported from a European country.
ACKNOWLEDGEMENTS
We thank all members of the Surgical Pathology Part, Department of Pathology, Seoul National University Hospital, Seoul, Korea for their help in the diagnosis of our case.
References
- 1. Eckert J, Gemmell MA, Meslin FX, Pawlowski ZS. WHO/OIE Manual on Echinococcosis in Humans and Animals: a Public Health Problem of Global Concern. 2001. Paris, France. World Organization for Animal Health; p. 1-262.
- 2. Chai JY, Seo M, Suh KS, Lee SH. An imported case of hepatic unilocular hydatid disease. Korean J Parasitol 1995;33:125-130.
- 3. Jung BH, Kim TH, Kang JS, Chang K, Jeong ET, Chae KM, Choi SH, Moon HB. A case of pulmonary and hepatic hydatid cystic disease. Korean J Med 1993;45:550-555. (in Korean).
- 4. Cho YJ, Chu JP, Jeong GS. A case of hydatid disease imported from possible endemic area. Program and Abstracts of the 38th Annual Meeting of the Korean Soc Parasitol. 1996. (in Korean).
- 5. Chae GR, Ann HS, Soo BJ, Chae KM. A clinical case report of hydatid disease of the liver and lung caused by Echinococcus granulosus. J Korean Surg Soc 1996;50:285-290. (in Korean).
- 6. Yoo CJ, Lee KS, Lee KG, Kwon OJ, Park HK. Cystectomy and hepatic resection for cystic lesion of the liver. J Korean Surg Soc 2001;61:516-523. (in Korean).
- 7. Kim JM, Choi KW, Lee HJ. A clinical case report of hydatid cyst of the liver. Yeungnam Univ J Med 2001;18:138-143. (in Korean).
- 8. Koh YS, Joo JK, Kim JC, Cho CK, Kim HJ. A clinical case report of hydatid cyst of liver. Korean J Hepatobiliary Pancreat Surg 2003;7:148-151. (in Korean).
- 9. Jeon SH, Kim TH, Lee HL. Laparoscopic treatment of isolated renal hydatid cyst. Korean J Urol 2007;48:555-557. (in Korean).
- 10. Jeoung KW, Ko YH, Kim HC, Wi JS, Moon JM, Chun BJ, Heo T, Min YI. A case of hydatid disease diagnosed in anaphylatic shock of unknown cause. J Korean Soc Emerg Med 2003;14:210-215. (in Korean).
- 11. Kim IK, Kim DY, Moon IS, Kim TS, Ock MS, Oh KS, Rhew HY. A case of echinococcal hydatid cyst as misdiagnosed to the bladder cancer. Korean J Urol 2004;45:1292-1295. (in Korean).
- 12. Ryou JY, Kim KH, Kim SY. Hydatid cyst of the orbit. J Korean Ophthalmol Soc 2006;47:484-488. (in Korean).
- 13. Kang MJ, Lee SH, Kim SJ, Chei YH, Park JH, Park DH, Park SH. A case of multiple intraperitoneal cysts from ruptured hepatic hydatid cysts. Korean J Gastroenterol 2007;50:203-206. (in Korean).
- 14. Kim IY, Kim SW, Shin HC, Han JK. US and CT findings of splenic hydatid cyst: a case report. J Korean Soc Ultrasound Med 2009;28:39-42.
- 15. Park KH, Jung SI, Jang HC, Shin JH. First successful puncture, aspiration, injection, and re-aspiration of hydatid cyst in the liver presenting with anaphylactic shock in Korea. Yonsei Med J 2009;50:717-720.
- 16. Suh JH, Kim YH. Pulmonary hydatid cyst found in a foreign worker from the endemic area: a case report. Korean J Thorac Cardiovasc Surg 2008;41:527-531. (in Korean).
- 17. Kang J, Chang JB, Bae LS, Kyu HS, Hyeon J, Hyup KS, Lee SE. A case of recurred hydatid cyst in pelvic cavity. Korean J Urol 1999;40:937-940. (in Korean).
- 18. Chung KY, Lee DY, Hong PW, Chung HJ, Choi IJ, Min DY. Surgical treatment of pulmonary hydatid cysts -two cases report-. Korean J Thoracic Surg 1983;16:518-525. (in Korean).
- 19. Nouir NB, Nunez S, Frei E, Gorcii M, Muller N, Gianinazzi C, Mekki M, Nouri A, Babba H, Gottstein B. Post-surgical follow-up (by ELISA and immunoblotting) of cured versus non-cured cystic echinococcosis in young patients. Parasitology 2008;135:105-114.
- 20. Chai JY. In: Ito A, Wen H, Yamasaki H, editors. Asian Parasitology. Echinococcosis in Korea. Vol. 2. Taeniasis/cysticercosis and echinococcosis in Asia. 2005. Chiba, Japan. Published by AAA Committee; p. 179-183.
- 21. Isshiki O. Studies on echinococcosis in Korean cattle. I. Occurrence and geographical distribution of bovine echinococcosis in Korea. Jpn J Vet Sci 1944;6:153-180. (in Japanese).
Fig. 1Ultrasonography of the patient. The liver cyst (arrows) shows a 'ball of wool' appearance.

Fig. 2Surgical specimen of the echinococcal cyst resected from the patient. A protruding large cystic mass (upper) is seen.

Fig. 3Gross photograph of the interior of the cyst. The cyst contains necrotic tissues, but without protruding masses or objects.
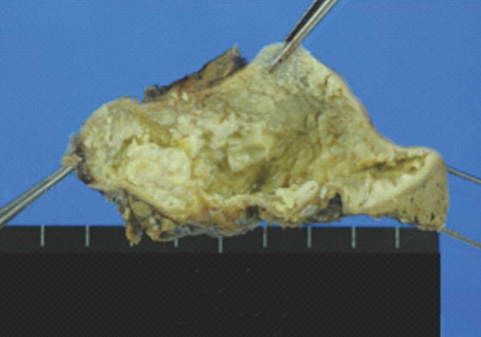
Fig. 4A degenerating protoscolex of Echinococcus granulosus showing 2 suckers (arrows) and necrotic background of the cyst. H-E stain, ×400.
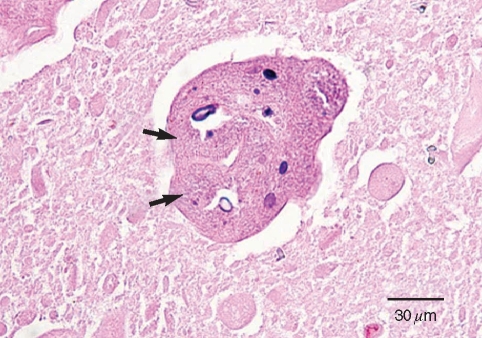
Fig. 5Another degenerating protoscolex of E. granulosus showing hooklets (arrow). H-E stain, ×600.
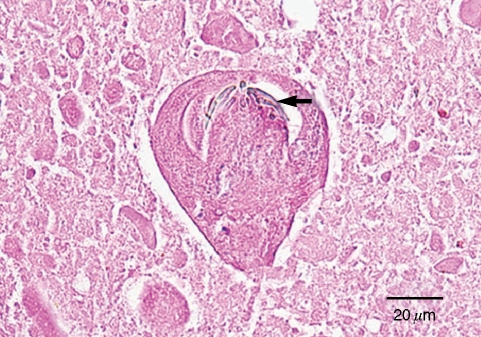
Fig. 6Freed (upper left) and grouped (center) hooklets of E. granulosus in the necrotic background, with the laminated cyst wall (long arrow) and the germinal layer (short arrow), which is a characteristic feature of hydatid cysts. H-E stain, ×400.
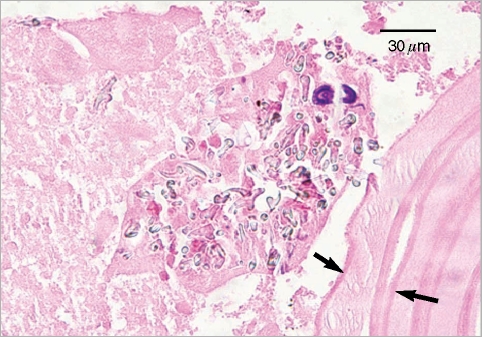
Fig. 7Freed protoscolices (arrows) of E. granulosus within the cyst. H-E stain, ×600.

Table 1.Brief summary of the 31 human echinococcosis cases reported in the Republic of Korea
Table 1.
|
Case No. |
Age & sex |
Chief complaints |
History of travel abroad |
Incubation perioda
|
Involved organ |
Reference |
|
Koreans |
|
|
|
|
|
|
|
1 |
27/F |
Chest pain |
None |
Uncertain |
Lung |
Reviewed [2], [18] |
|
2 |
25/M |
Chest pain |
Kuwait |
3 years |
Lung |
Reviewed [2], [18] |
|
3 |
31/M |
Asymptomatic |
Middle East |
4 years |
Lung |
Reviewed [2] |
|
4 |
30/M |
Chest pain |
Middle East |
6 months |
Lung |
Reviewed [2] |
|
5 |
32/M |
Epigastric discomfort |
Saudi Arabia |
5 years |
Liver |
Reviewed [2] |
|
6 |
39/M |
Epigastric discomfort |
Saudi Arabia |
3 years |
Liver |
Reviewed [2] |
|
7 |
49/M |
Pleurisy symptoms |
Saudi Arabia |
21 months |
Lung |
Reviewed [2] |
|
8 |
25/M |
Epigastric pain, wt. loss |
Pakistan |
2 years |
Liver |
Reviewed [2] |
|
9 |
39/M |
Epigastric discomfort |
Saudi Arabia |
11 years |
Liver |
Reviewed [2] |
|
10 |
33/M |
Abdominal discomfort |
Saudi Arabia |
6 years |
Liver, peritoneal cavity |
Reviewed [2], recurred [17] |
|
11 |
26/M |
Chest mass |
Libya |
2 years |
Lung |
Reviewed [2] |
|
12 |
39/M |
General malaise |
Saudi Arabia |
11 years |
Lliver |
Reviewed [2] |
|
13 |
44/M |
Asymptomatic |
Saudi Arabia |
7 years |
Lung |
Reviewed [2] |
|
14 |
55/M |
Epigastric discomfort |
Middle East |
10 years |
Liver |
Reviewed [2] |
|
15 |
43/M |
Epigastric discomfort |
Saudi Arabia |
> 4-5 years |
Liver |
Reviewed [2] |
|
16 |
38/M |
Indigestion |
Saudi Arabia |
3 years |
Liver |
[2] |
|
17 |
50/M |
Abdominal discomfort |
Saudi Arabia, Iraq |
1 year |
Liver, lung |
[3] |
|
18 |
27/F |
Abdominal pain |
China |
1 year |
Liver |
[4] |
|
19 |
53/M |
Bloody sputum |
Middle East |
12 year |
Liver, lung |
[5] |
|
20 |
53/M |
Abdominal pain |
Middle East |
Unknown |
Liver |
[6] |
|
21 |
49/M |
Asymptomatic |
Brazil |
Unknown |
Liver |
[6] |
|
22 |
52/M |
Liver mass |
Vietnam |
33 years |
Liver |
[7] |
|
23 |
66/M |
General malaise |
Saudi Arabia |
> 30 years |
Liver |
[8] |
|
24 |
56/F |
Dizziness |
Unknown |
1-8 years |
Kidney |
[9] |
|
Uzbek |
|
|
|
|
|
|
|
1 |
31/M |
Syncope |
Uzbekistan |
Uncertain |
Liver |
[10] |
|
2 |
38/M |
Abdominal pain |
Uzbekistan |
Uncertain |
Bladder |
[11] |
|
3 |
33/F |
Exophthalmos |
Uzbekistan |
Uncertain |
Orbit |
[12] |
|
4 |
35/M |
Abdominal pain |
Uzbekistan |
Uncertain |
Liver, peritoneal cavity |
[13] |
|
5 |
28/M |
Abdominal discomfort |
Uzbekistan |
Uncertain |
Spleen |
[14] |
|
6 |
30/M |
Syncope |
Uzbekistan |
Uncertain |
Liver |
[15] |
|
Mongolian |
|
|
|
|
|
|
|
1 |
34/M |
Chest discomfort |
Mongolia |
Uncertain |
Lung |
[16] |









