Abstract
Toxocariasis is one of the most common geohelminth infections in several parts of the world. We describe a rare case of ocular toxocariasis with secondary exudative retinal detachment treated with albendazole and an intravitreal dexamethasone implant. A 13-year-old boy with counting finger vision was diagnosed with retinal vasculitis and exudative retinal detachment in his right eye. Fundoscopic examination revealed retinal hemorrhage, retinal vasculitis, and exudative retinal detachment. Serological test using serum and intraocular aqueous humor were positive for anti-Toxocara specific IgG antibodies. He received repeated doses of intravitreal dexamethasone implants combined with oral albendazole. A sequential follow-up optical coherence tomography revealed that the retina was successfully reattached. His visual acuity subsequently improved to 20/400.
-
Key words: Ocular toxocariasis, retinal detachment, treatment, dexamethasone, albendazole
INTRODUCTION
Toxocariasis is one of the most widely reported zoonotic helminthiasis globally. It is especially common in subtropical and tropical regions, and in poor hygiene communities of some countries. Larvae of
Toxocara canis, the common roundworm found in dogs, and the larval stages of
Toxocara cati, the roundworm found in cats, can cause toxocariasis [
1]. Human infection occurs in 5 ways: visceral larva migrans (VLM) syndrome, ocular larva migrans (OLM) syndrome, covert toxocarosis, common toxocarosis (comT), and neurotoxocarosis (NT) [
2]. Ocular disease is caused by the migration of
Toxocara larvae through blood vessels into the circulatory system, which finally infected to the posterior section of the eye [
3]. The main signs of ocular toxocariasis (OT) include subretinal granulomatous mass/scar, vitritis, and scotoma. The primary treatment modalities are steroids, antiparasitic drugs, and surgery [
4].
Dexamethasone (DEX) is a strong synthetic member belonging to the glucocorticoid class of steroid drugs. DEX exhibits anti-inflammatory and immunosuppressant activities 30 times higher than those of cortisol and 6 times higher than those of triamcinolone [
5]. The DEX implant is an approved therapy for the diabetic macular edema, cystoid macular edema secondary to retinal vein occlusion, and non-infectious posterior uveitis [
6]. The most common adverse ocular reactions that may appear are increased intraocular pressure (IOP) and onset or progression of cataract [
7]. In the present study, we treated the patient with repeated injections of DEX implant and short-term oral administration of albendazole. To the best of our knowledge, this is the first case report describing the success in relieving inflammation of ocular toxocariasis following intravitreal implantation of DEX.
CASE DESCRIPTION
A 13-year-old male patient was presented to a local clinic with the complaints of progressively decreasing vision in the right eye for 1 month, with no febrile and gastrointestinal symptoms, such as nausea and diarrhea. The patient was residing in a village and had a long history of contact with animals, especially dogs. He had no personal or family history of systemic or ocular disease. The patient was diagnosed with retinal detachment in the right eye by a local ophthalmologist. We advised him to exclude rheumatic immune diseases from the diagnosis. After consultation, the patient’s immune function was found to be normal. The visual acuity of the right eye decreased to counting fingers. The patient was then transferred to our hospital.
Upon examination, his visual acuity was counting fingers in the right eye (not corrected) and 20/12 in the left eye. His intraocular pressure was 14 and 13 mmHg in the right and left eye, respectively. Fundus examination of the right eye revealed subretinal hemorrhage, yellow-white exudates with exudative retinal detachments, and dilated and tortuous vessels.
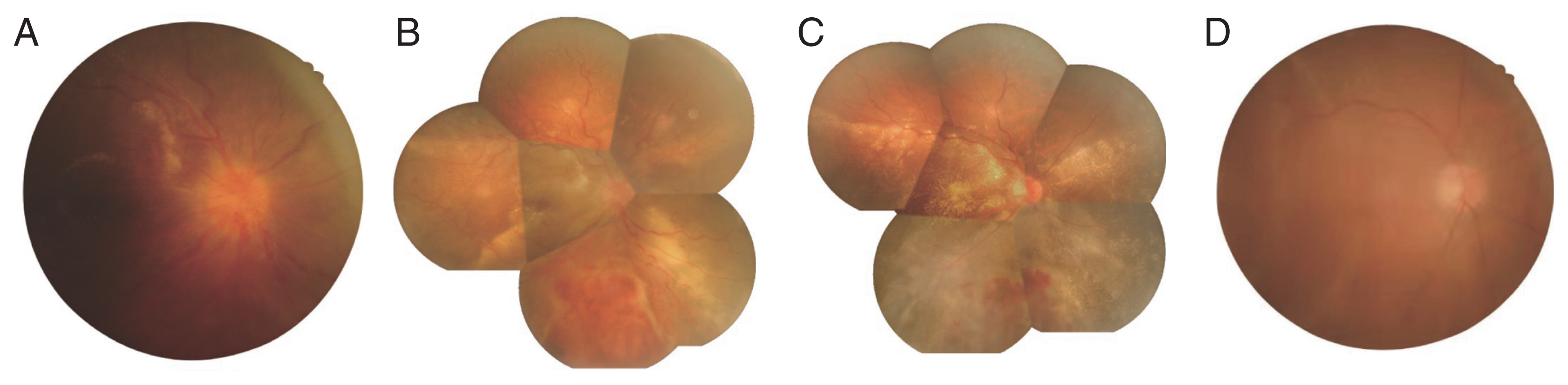
Fundus examination revealed the presence of exudate around the blood vessels in the macular area, edematous optic disc, dilated and tortuous retinal veins, and preretinal hemorrhages in the inferior retina (
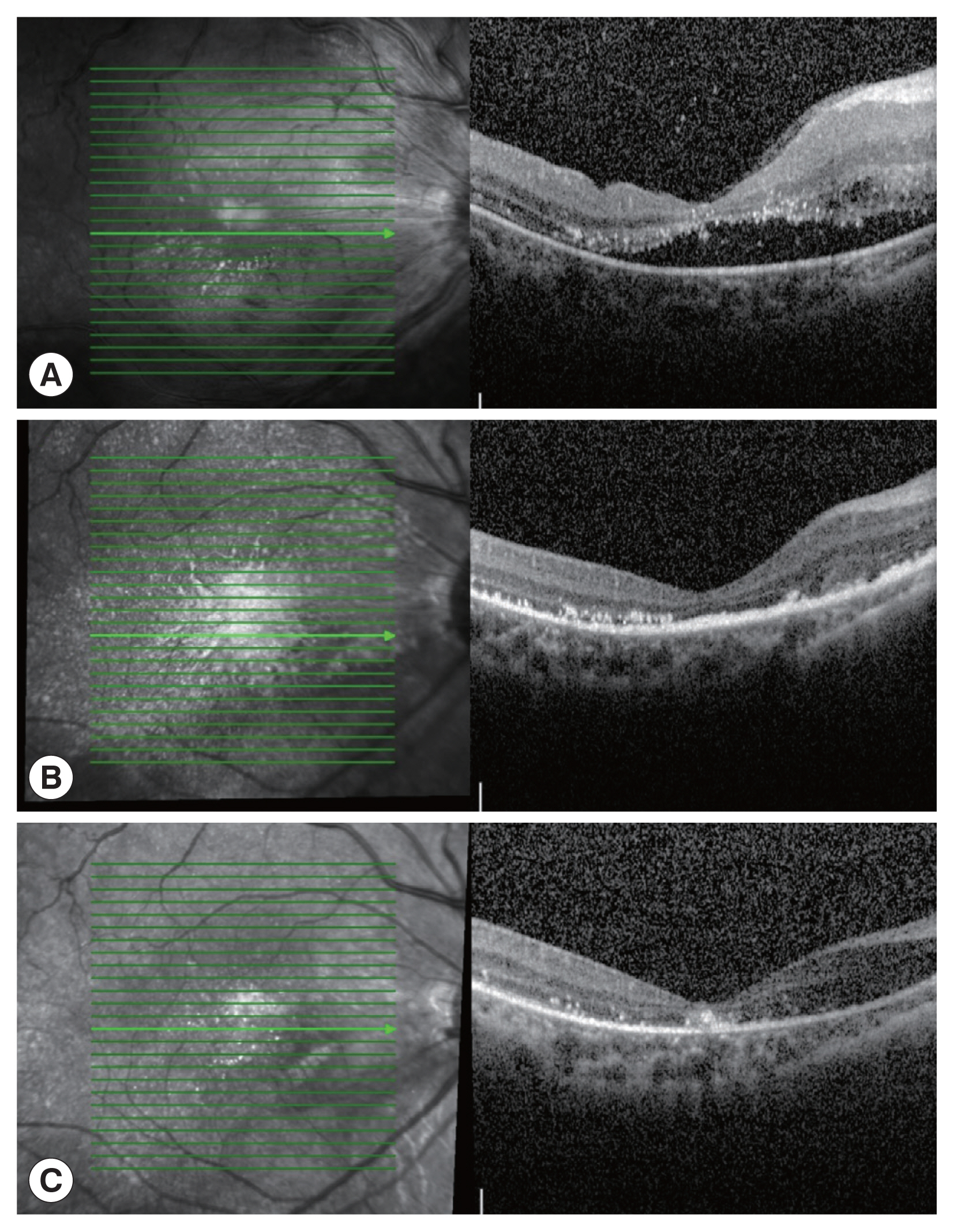
Fig. 1A). An anterior segment optical coherence tomography (OCT) image revealed neurosensory detachment (
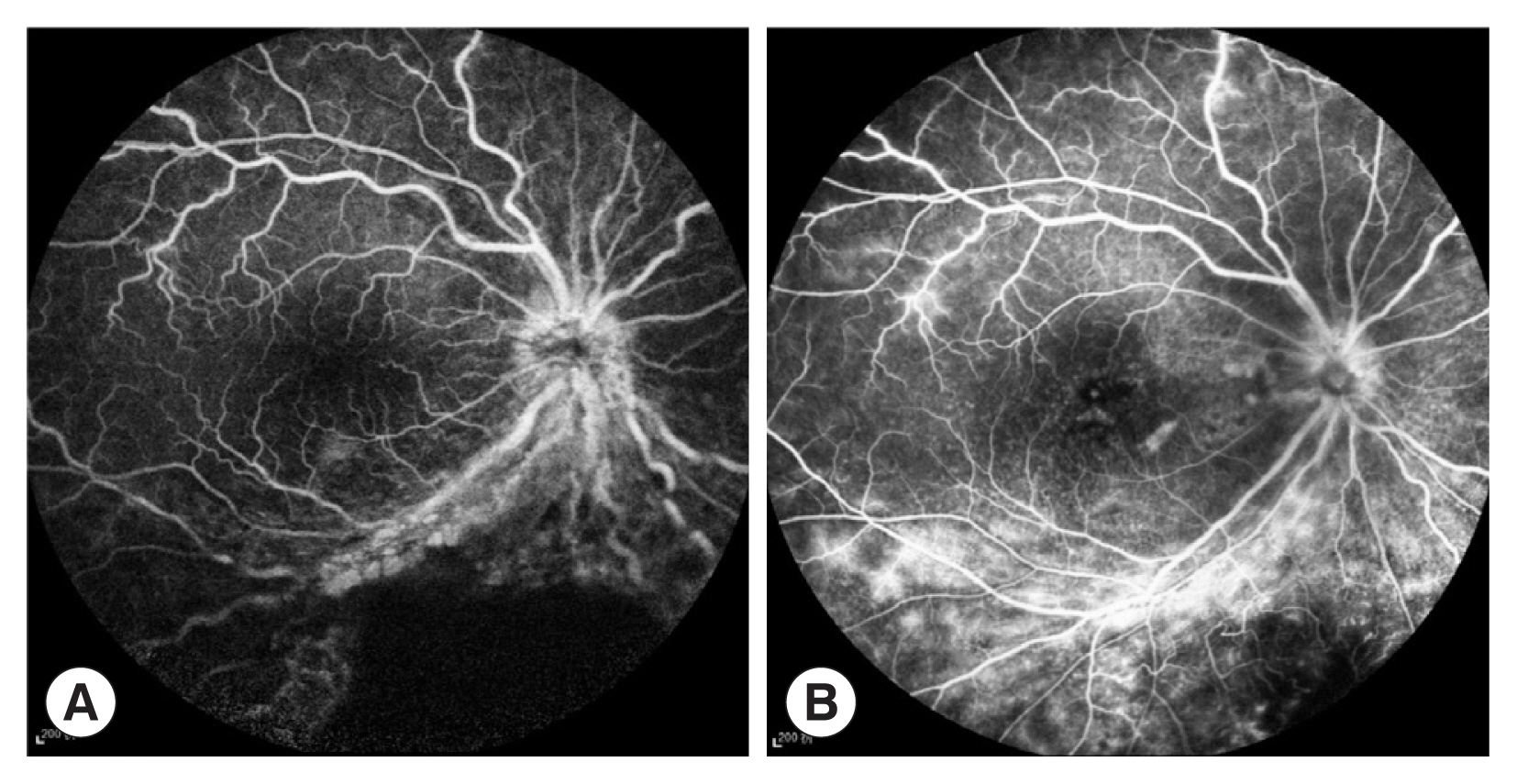
Fig. 2A). Fundus fluorescein angiography (FFA) revealed hypofluorescence area, corresponding to the hemorrhage focus inferior to the disc. Dilatation of disc vessel was observed, which was accompanied by retinal vascular tortuosity and leakage of the fluorescent tracer (
Fig. 3A).
A complete blood cell count analysis indicated absence of leukocytosis or eosinophilia, and parasitological examination of stools did not reveal parasitic propagules. There was no abnormality on the chest CT and ultrasound scan of the major organs. Initially, we suspected that the patient contracted a viral infection. He was treated with the antiviral drug ganciclovir systemically and ganciclovir gel for the right eye. After 2 days of treatment, the blurred vision of the patient did not significantly improve. The patient’s past history revealed that he was in contact with dogs for a long period who had never vaccinated. Therefore, enzyme-linked immunosorbent assay (ELISA) tests were conducted on both the serum and vitreous humor. Laboratory investigations revealed an increase in serum IgG anti-Toxocaria antibody levels (51.72 U; reference range IgG negative: <9 U), and vitreous humor (3.21 U; reference range IgG negative: <3 U). The Goldmann–Witmer coefficient was 2.92, which was higher than the normal value. A diagnosis of Toxocara chorioretinitis combined with exudative retinal detachment was made based on the patient’s clinical appearance and laboratory examination results. The antiviral medication was immediately terminated.
The patient was treated with albendazole 400 mg daily for 5 days as laboratory investigations confirmed infection with toxocariasis. He was administered the first injection of intravitreal DEX implants. At 1-week post-DEX implant injection, fundus examination showed an improved disc edema (
Fig. 2B). Neuroepithelial layer detachment was recovered, and the retinal exudates was decreased in OCT images (
Fig. 2B).
At 1-month post-DEX implant injection, a slit-lamp examination revealed that the anterior segment was normal. There was no sign of cataract and inflammation. His IOP was 16 mmHg, and best-corrected visual acuity (BCVA) was 0.05. On fundus examination, we observed improvement of inferior retinal detachment, retinal telangiectasis, and hemorrhage. The exudate was absorbed (
Fig. 1C).
At 8 months post-DEX implant injection, the patient had a BCVA of 20/400 and IOP of 16 mmHg. The fundus examination revealed retinal blood vessel whitening and slightly edematous inferior retina (
Fig. 1D). OCT showed that the subretinal exudation was improved significantly (
Fig. 2C). Retinal hemorrhage and vascular tortuosity were improved. Retinal exudation was decreased in FFA (
Fig. 3B). Next day, we administered the injections of intravitreal DEX implant again to the patient.
Due to the COVID-19 epidemic, the patient and his family had difficulty to visit our hospital for follow-up on time. We thus recommended regular check-ups at local hospitals. When regular follow-up calls were conducted, the patient complained no sign of new discomfort or adverse events in his right eye.
DISCUSSION
Toxocariasis is a neglected worm-infecting disease that primarily affects young children and adolescents. OT is a clinical manifestation of intraocular infection by the second-stage larvae of
Toxocara species, which causes significant vision loss. The main reasons behind vision loss are vitritis, cystoid macular edema, and traction retinal detachment [
8]. To the best of our knowledge, this is the first report on the application of DEX implant in OT patients.
The diagnosis and treatment of OT are usually based on the history of exposure, clinical manifestations, laboratory tests, imaging studies, and immunological tests. In China,
T. canis is the most common parasite to invoke human infection [
9]. OT is usually considered as a unilateral disease that typically presents with retinal granuloma, a yellowish or whitish inflammatory mass, in the posterior segment or peripheral retina. OT also has many atypical presentations [
10]. When unusual appearances of exudative retinal detachment occur in the patient, we should consider the possibility of helminth infection. Tracing the history of residence and exposure to cats or dogs, relevant antibody tests should be conducted. The overall seroprevalence in Chinese children is 19.3%, which should be concerning for the government [
9].
OT can be treated either medically or surgically. The main standard treatment of OT includes corticosteroid administration in patients combined with deworming treatment to achieve desired outcomes [
10]. Many applications of local or systemic corticosteroids in patients with OT have been reported. Corticosteroids are commonly administered via the oral route with topical administration [
11,
12]. Two reports described the cases of choroidal neovascularization (CNV) secondary to OT treated successfully with intravitreal injections of anti-vascular endothelial growth factor (VEGF) agents [
13,
14]. However, it has limited efficacy in addressing the structural retinal complications. Retinal detachment, retinal anterior membrane, and persistent vitreous opacities are common surgical indications for pars plana vitrectomy (PPV). However, PPV has many potential complications, such as cataract progression and iatrogenic breaks [
15]. Moreover, close postoperative monitoring is highly required. Our patient experienced exudative retinal detachment, and the treatment reduced the risks of vitrectomy and burden on patient for follow-up. Additionally, a successful PPV outcome, defined as anatomic success, is 50% in patients with retinal detachment secondary to OT [
16]. Our patient achieved anatomic success with retinal reattachment. However, more treatment cases are needed to establish the success rate of post-DEX implant injection in OT patients.
Additionally, the action timeframe of DEX implant is up to 4–6 months, which differs from other partial corticosteroid injections reported in previous studies [
17]. Moreover, after corticosteroid injections, such as triamcinolone, retinitis reoccurs in 3–4 months. Our patient showed no recurrence of retinal detachment or retinal vasculitis even after 8 months post DEX implant injection. Meanwhile, a combination treatment with albendazole and oral steroids to reduce the recurrence of inflammation was prescribed [
16]. It should be noted that this conclusion was made only in patients who were administered oral steroids. However, the application of albendazole and DEX implant on the recurrence of OT inflammation requires longer follow-up and more research.
Unfortunately, visual acuity was severely affected in our patient. Visual loss may not be diagnosed timely in pediatric patients. Therefore, when the patient finally notices it, the stage of the inflammatory process has already advanced, and vision loss may become permanent. After the treatment, the anatomy of the retina of our patient’s fundus was restored, the inflammation in the eye was reduced, but his functional vision did not improve significantly.
OT is a frequently neglected form of helminth infection. It is important to prescribe an appropriate treatment depending on different manifestations of this disease. This is the first reported case of successful treatment using an intravitreal DEX implant (Ozurdex®) for retinal detachment secondary to OT. No adverse event was reported during the follow-up period. A combined treatment with albendazole and DEX implant injection may be considered as an effective and safe approach for OT with exudative retinal detachment.
Notes
-
Consent for publication
Written and signed consent from the patient’s parent involved in this report was obtained for the publication of their personal and clinical details along with any identifying images to be published in this study.
The data generated during the present study is available upon request from the corresponding author.
-
The authors declare that they have no competing interests.
ACKNOWLEDGMENTS
The case report did not require ethical approval. Written informed consent was obtained from the patient for the surgical procedure.
Fig. 1(A) Fundus photograph revealed exudate around the macular area, edematous optic disc, dilated and tortuous retinal veins, and preretinal hemorrhages during the initial presentation. No granuloma was found. (B) Disc edema improved; however, retinal hemorrhages remained 1 week post injection. (C) Retinal hemorrhages and exudates were absorbed, and vascular tortuosity was improved compared to 1 month after injection. (D) In 8 months follow-up, the retina was flat. No hemorrhages, exudates, and granulomas were observed.
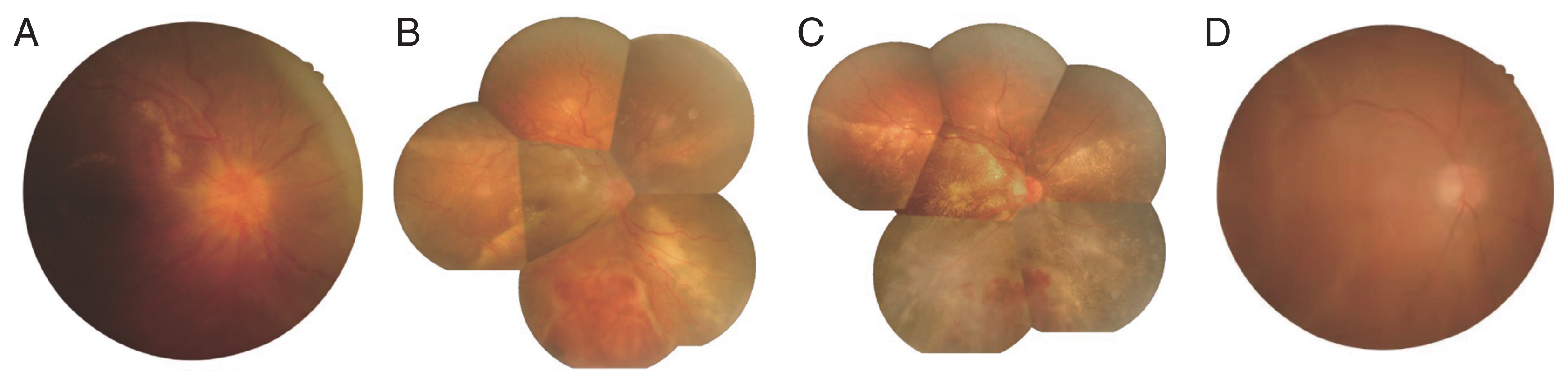
Fig. 2(A) A hyporreflective area between the neuroepithelium and pigment epithelium in the macular area was observed. (B) The retina was reattached, while retinal exudates remained 1 month post injection. (C) Subretinal exudation improved significantly 8 months post-injection.
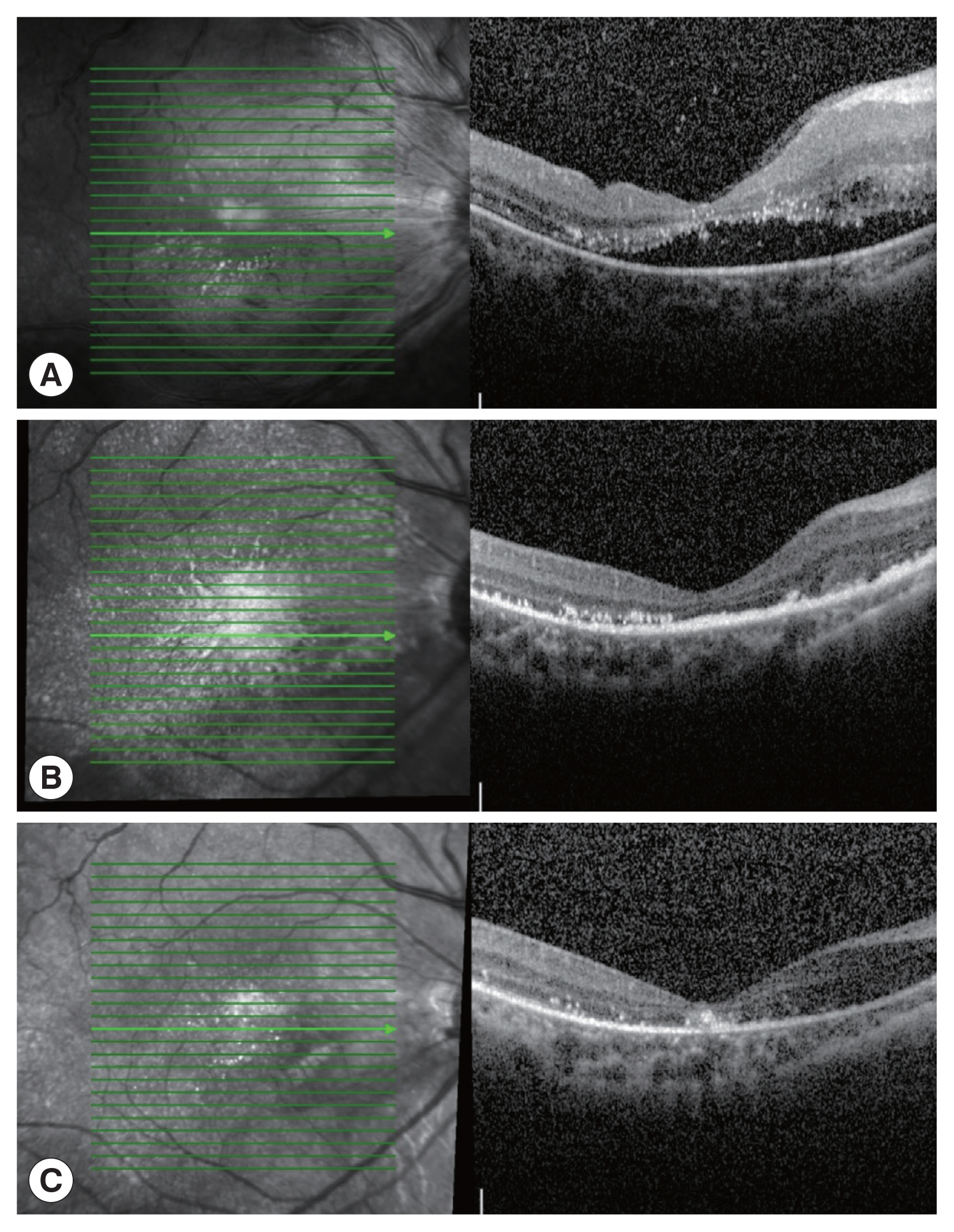
Fig. 3(A) Fundus fluorescein angiography (FFA) showed hypofluorescence areas corresponding to the hemorrhagic sites. The optic disc capillaries and retinal vessels were found to be tortuously dilated during initial presentation. (B) Retinal hemorrhage was absorbed, vascular tortuosity was improved, and retinal exudation was decreased at 8 months post-injection.
References
- 1. Chen J, Liu Q, Liu GH, Zheng WB, Hong SJ, Sugiyama H, Zhu XQ, Elsheikha HM. Toxocariasis: a silent threat with a progressive public health impact. Infect Dis Poverty 2018;7:59. https://doi.org/10.1186/s40249-018-0437-0
- 2. Auer H, Walochnik J. Toxocariasis and the clinical spectrum. Adv Parasitol 2020;109:111-130. http://doi.org/10.1016/bs.apar.2020.01.005
- 3. Taylor MR. The epidemiology of ocular toxocariasis. J Helminthol 2001;75:109-118.
- 4. Woodhall D, Starr MC, Montgomery SP, Jones JL, Lum F, Read RW, Moorthy RS. Ocular toxocariasis: epidemiologic, anatomic, and therapeutic variations based on a survey of ophthalmic subspecialists. Ophthalmology 2012;119:1211-1217. https://doi.org/10.1016/j.ophtha.2011.12.013
- 5. Scaramuzzi M, Querques G, Spina CL, Lattanzio R, Bandello F. Repeated intravitreal dexamethasone implant (Ozurdex) for diabetic macular edema. Retina 2015;35:1216-1222. https://doi.org/10.1097/iae.0000000000000443
- 6. Fassbender Adeniran JM, Jusufbegovic D, Schaal S. Common and rare ocular side-effects of the dexamethasone implant. Ocul Immunol Inflamm 2017;25:834-840. https://doi.org/10.1080/09273948.2016.1184284
- 7. Hostovsky A, Muni RH, Eng KT, Mulhall D, Leung C, Kertes PJ. Intraoperative dexamethasone intravitreal implant (Ozurdex) in vitrectomy surgery for epiretinal membrane. Curr Eye Res 2020;45:737-741. https://doi.org/10.1080/02713683.2019.1697454
- 8. Stewart JM, Cubillan LD, Cunningham ET Jr. Prevalence, clinical features, and causes of vision loss among patients with ocular toxocariasis. Retina 2005;25:1005-1013. https://doi.org/10.1097/00006982-200512000-00009
- 9. Kong L, Peng HJ. Current epidemic situation of human toxocariasis in China. Adv Parasitol 2020;109:433-448. https://doi.org/10.1016/bs.apar.2020.01.016
- 10. Ahn SJ, Ryoo NK, Woo SJ. Ocular toxocariasis: clinical features, diagnosis, treatment, and prevention. Asia Pac Allergy 2014;4:134-141. https://doi.org/10.5415/apallergy.2014.4.3.134
- 11. Jee D, Kim KS, Lee WK, Kim W, Jeon S. Clinical features of ocular toxocariasis in adult Korean patients. Ocul Immunol Inflamm 2016;24:207-216. https://doi.org/10.3109/09273948.2014.994783
- 12. Pak KY, Park SW, Byon IS, Lee JE. Ocular toxocariasis presenting as bilateral scleritis with suspect retinal granuloma in the nerve fiber layer: a case report. BMC Infect Dis 2016;16:426. https://doi.org/10.1186/s12879-016-1762-1
- 13. Yoon DY, Woo SJ. Intravitreal administration of ranibizumab and bevacizumab for choroidal neovascularization secondary to ocular toxocariasis: a case report. Ocul Immunol Inflamm 2018;26:639-641. https://doi.org/10.1080/09273948.2016.1239744
- 14. Lyall DAM, Hutchison BM, Gaskell A, Varikkara M. Intravitreal Ranibizumab in the treatment of choroidal neovascularisation secondary to ocular toxocariasis in a 13-year-old boy. Eye (Lond) 2010;24:1730-1731. https://doi.org/10.1038/eye.2010.131
- 15. Znaor L, Medic A, Binder S, Vucinovic A, Marin Lovric J, Puljak L. Pars plana vitrectomy versus scleral buckling for repairing simple rhegmatogenous retinal detachments. Cochrane Database Syst Rev; 2019. 3:CD009562 https://doi.org/10.1002/14651858.CD009562.pub2
- 16. Ahn SJ, Woo SJ, Jin Y, Chang YS, Kim TW, Ahn J, Heo JW, Yu HG, Chung H, Park KH, Hong ST. Clinical features and course of ocular toxocariasis in adults. PLoS Negl Trop Dis 2014;8:e2938. https://doi.org/10.1371/journal.pntd.0002938
- 17. Takakura A, Tessler HH, Goldstein DA, Guex-Crosier Y, Chan CC, Brown DM, Thorne JE, Wang R, Cunningham ET Jr. Viral retinitis following intraocular or periocular corticosteroid administration: a case series and comprehensive review of the literature. Ocul Immunol Inflamm 2014;22:175-182. https://doi.org/10.3109/09273948.2013.866256