Abstract
The characteristics of vivax malaria epidemics along the demilitarized zone (DMZ) in the Republic of Korea has been established by the early surveillance data. To further characterize the epidemic, data of civilian patients microscopically diagnosed with malaria from 1995 through 2000 were analyzed in Yonchon-gun (county). Malaria incidence was greater in male civilians > 30 years of age (p < 0.05). The annual parasite index was significantly higher in those living in the administrative areas (Myeon) traversed by DMZ than those living in Myons not traversed by DMZ (p < 0.05). Analysis according to the distance (4 to 14 km) from DMZ showed that people living in villages close to DMZ had higher annual parasite indices than those living in villages remote from DMZ (p for trend < 0.05). Civilians living in Myeons with plains and located in northwestern part of the county had higher annual parasite indices than those living in hilly Myeons located in southeastern part of the county (p for trend < 0.05). These findings suggest that the contraction of vivax malaria is related with night-time outdoor activities, and that the distance from DMZ is a risk factor. In this area, the flying distance of infected vector mosquitos can explain the annually repeating occurrence of civilian cases.
-
Key words: Plasmodium vivax, vivax malaria, epidemiology, Korea
INTRODUCTION
In 1993, a patient of vivax malaria was diagnosed in a northern county of Kyonggi-do, Republic of Korea (ROK). In the subsequent years, the incidence of malaria patients showed a typical epidemic pattern (
Chai, 1999;
Ree, 2000). Since 1998, the total number of reported cases of vivax malaria stabilized (approximately 4,000 cases/year), and might be related with increased use of chemoprophylaxis in army personnel assigned to "high risk" areas and local health education (
Ree, 2000;
Park et al., 2000;
Park et al., 2001). Although the number of reported malaria patients is not increasing as steeply as those in the previous seven years, the epidemiology in 2000 showed the following tendencies: (1) the malaria-risk areas are spreading east and west along the demilitarized zone (DMZ) and (2) the number of civilian cases is increasing, when compared with that of military cases. These findings have raised a question whether the secondary transmissions are occurring In the risk areas (
Park et al., 2000,
2001).
The source of the present malaria epidemic is yet to be definitely established. It is mainly due to the non-availability of malaria statistics in the other side of DMZ. However, we can conclude definitely that the origin is somewhere inside the East Asia. A genetic study of circumsporozoite protein in isolates of
Plasmodium vivax, causing the present epidemic, revealed two genotypes (SK-A and SK-B), both of which are similar to Chinese and North Korean strains (
Kho et al., 1999b). In addition, the borderline character of the present epidemics has been described by Lee et al. (
1998) and Kho et al. (
1999a). By dotting a map of the most probable places of malaria contraction of both military and civilian cases of malaria, Kho et al. (
1999a) clearly showed that all the patients had contracted malaria when residing within 20 km from DMZ.
In controlling the present epidemic, the issues on the source of infection and secondary transmission of malaria are important because they are closely related with the policy and prospect of control. This study was undertaken for the further analysis of the incidence patterns of vivax malaria in civilians residing in a high-risk county of Kyonggi-do.
MATERIALS AND METHODS
Geographical characteristics of the study county
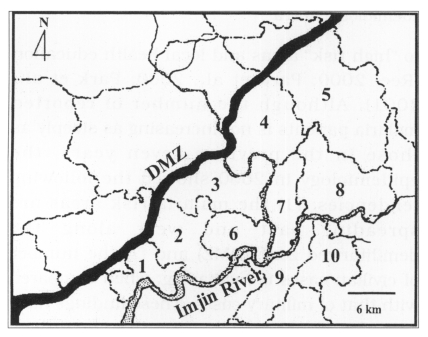
The study area, Yonchon-gun, is a known high-risk county of the present vivax malaria epidemic in ROK, and is located in the northeast corner of Kyonggi-do (latitude 37°57' /38°16'; longitude 126°39' /127°10'). It consists of administrative areas of eight Myons and two Eups (
Fig. 1). The total area of the county is 625 km
2. The Imjin River flows from the north to the south through Chung and Kunnam and then turns westward along the southern border of the county, dividing the county into the southern and eastern hilly parts and northern and western plain parts. The population of the county is 53,776 (December 1999). Since the 1953 Armistice, the 4-km wide DMZ runs diagonally from the northeast to the southwest through five Myeons, and divides the county into the south and north. The ROK Government administers the south. Due to its strategic location, a zone of several kilometers distance along the southern border of DMZ is controlled by ROK Army, and civilians can manage their farmland within the zone only by permission. Yonchon-gun has been one of the ecologically preserved areas in Korea. Light-trap collections of mosquitos indicated that > 40% of all mosquitos collected are
Anopheles sinensis, the principal malaria vector in ROK (
Shim et al., 1997).
The ROK Communicable Disease Prevention Act designates malaria as third category disease, which means that hospitals and clinics should report the occurrence of microscopically diagnosed cases to local health centers. Because of public concerns over the current epidemic, and the free government supply of antimalarial drugs to any microscopically diagnosed case, the report rate has been almost 100% since the beginning of the epidemic.
Receiving the reports, the health centers confirm the species of Plasmodium in blood smear, and then collect demographic information of the patients, such as name, sex, age, and address, together with clinical data, including symptoms, dates of clinical onset and diagnosis, and histories of travelling abroad, blood transfusion, and use of narcotics. Civilians with a recent history of travelling abroad, and possible syringe infections or civilians that were diagnosed as malaria after discharge from military service in high-risk areas (two cases in 1999 and four in 2000) were excluded from this study.
Statistical analysis
Local population data were used as denominators in calculating annual parasite indices (API, number of malaria patients divided by population multiplied by 1,000) by age, Myeon, and village. The differences in API among the age groups were examined by χ2-test. The differences in API between the administrative Myeons traversed by DMZ and those not traversed by DMZ, and between flat Myeons and hilly Myeons (those located to the east of the Imjin River except Kunnam) were also examined by χ2-test. The differences in API according to the distance from DMZ were examined by Mantel-Haentzel χ2-test for trend. A p < 0.05 was regarded as significant.
RESULTS
Annual incidence and Incidence by age and sex
The total number of reported malaria cases among the civilian population was 647 from 1995 through 2000 (
Table 1). During that period, proportion of males (420/27,608) with malaria was significantly greater than for females (227/ 26,158) (χ
2 = 39.91, p < 0.0001). Additionally males were at significantly greater risk annually for 1998 (χ
2 = 29.93, p < 0.0001), 1999 (χ
2 = 14.98, p < 0.0001) and 2000 (χ
2 = 5.16, p = 0.0232) (
Table 1).
The number of malaria patients for various age groups was significantly different in 1998 (χ
2 = 33.50, p < 0.0001), 1999 (χ
2 = 56.22, p < 0.0001) and 2000 (χ
2 = 78.76, p < 0.0001) (
Table 2). The age distribution of the malaria patients was greater for age groups > 30 years, with the age groups of 40-59-years-old having the highest API. The APIs in the years 1995, 1996 and 1997 were not analysed because of many zero incidences.
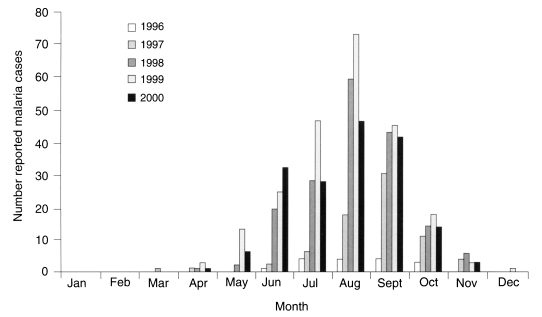
Monthly incidences of civilian cases of vivax malaria in Yonchon-gun are shown in
Fig. 2. During the six years from 1995 through 2000, the total monthly incidence was 0 in January and February, 1 in March, 6 in April, 21 in May, 78 in June, 112 in July, 200 in August, 159 in September, 57 in October, 12 in November, and 1 in December when the date of diagnosis was regarded as the date of incidence.
Overall, during the six years of epidemic, the average civilian API was 2.005 throughout the county. The API in the Myeons traversed by DMZ were compared with those in Myeons and Eups not traversed by DMZ (
Table 3). The APIs were significantly different between the two groups of administrative areas in 1998 (χ
2 = 25.73, p < 0.001), 1999 (χ
2 = 92.99, p < 0.0001) and 2000 (χ
2 = 26.84, p < 0.0001), and were greater in the Myeons traversed by DMZ.
The APIs in the Myeons with mostly plain areas were compared with those in hilly Myeons and Eups. Except for Kunnam, Myeons with plain areas were located in west of the Imjin River. API were significantly different between the two groups of plain and hilly administrative areas in 1998 (χ2 = 135.62. p < 0.0001), 1999 (χ2 = 219.17, p < 0.0001), and 2000 (χ2 = 112.34, p < 0.0001). The APIs in the years 1995, 1996 and 1997 were not analysed because of many zero incidences.
API in relation with the distance from DMZ
In high-risk Myeons, annual incidence and API for 22 villages were analysed based on the distance from DMZ, using 1998-2000 data (
Table 4). Using a map, the direct distance was measured from DMZ to the center of each village. For Changnam villages (range 4-8 km from DMZ), API was not significantly different based on the distance (χ
2for trend = 1.76, p = 0.891 in 1998, χ
2for trend = 0.05, p = 0.822 in 1999, χ
2for trend = 0.122, p = 0.727 in 2000, χ
2for trend = 0.0063, p = 0.937 in 1998-2000). For Paikhak villages (range 5-12 km from DMZ), API was not significantly different according to the distance In each year of 1998 (χ
2for trend = 1.79, p = 0.180), of 1999 χ
2for trend = 3.66, p = 0.056) and of 2000 (χ
2for trend = 2.13, p = 0.144), However, the average API from 1998 through 2000 was a significantly different based on the distance χ
2for trend = 7,489, p = 0,0062). For Wangjing villages, API were significantly different according to the distance each year and during the total period χ
2for trend = 2.92, p = 0.046 in 1998, χ
2for trend = 6.72, p = 0.0095 in 1999, χ
2for trend = 4.82, P = 0.282 in 2000, and χ
2for trend = 1.76, p = 0.891 in 1998-2000). For Kunnam villages, API were also significantly different according to the distance each year and during the total period (χ
2for trend = 22.23, p < 0.0001 in 1998, χ
2for trend = 25.45, p < 0.0001 in 1999, χ
2for trend = 23.15, p < 0.0001 in 2000, and χ
2for trend = 68.54, p < 0.0001 in 1998-2000).
For all 22 villages, API were significantly different according to the distance from DMZ each year as well as during the total period χ2for trend = 15.36, p < 0.0001 to 1998, χ2for trend = 33.89, p < 0.001 in 1999, χ2for trend = 10.71, p = 0.011 in 2000, and χ2for trend = 57.61, p < 0.0001 during 1998-2000).
DISCUSSION
In the current epidemic of vivax malaria, the incidence was higher in male civilians > 30 years of age in the high-risk county. API in those living in the Myeons traversed by DMZ was higher than that in those living in Myeons not traversed by DMZ. Analysis according to the distance from DMZ showed that people living in villages close to DMZ had higher API than those living in villages remote from DMZ. Civilians living in Myeons with plains and located in western part of the county had higher API than those living in hilly Myeons located in eastern part of the county.
National surveillance data for civilian malaria patients (
Lee et al., 1998) showed that male patients in their 20s accounted for the largest proportion of the reported cases and even in a non-malarious Province (
Kim, 2001). In most cases, those civilians were diagnosed as malaria after being retired from their military services in high-risk areas. Unlike the national data, the present analysis in a high-risk county showed that males > 30 years of age were at greater risk of contracting malaria. This skewed incidence pattern among the whole population, in terms of age and sex of the civilian cohorts, suggests that the contraction of malaria is a result of interactions between mosquitoes and civilians.
Anopheles sinensis, the principal vector of the local
P. vivax, has been known as a zoophilic, outdoor and night-time biter (
Ree, 2000), Presumably, if adult males among the farm villages have more outdoor activities during evening, i.e., fishing and social drinking after work-related activities during the malaria transmission season than other age or sex groups, they would be at increased risk. This presumption remains to be confirmed by future anthropologic surveys. The increased risk with outdoor evening activities (e.g., guard and patrol) has been shown for ROK soldiers stationed along the DMZ (
Kho et al., 1999a;
Park et al., 2000).
Because of fluctuating annual precipitation, and many other epidemiological factors including different behavioral patterns of population in relation with malaria contraction and prevention, API in high-risk villages were fluctuating annually. In the present study, however, the malaria incidence was shown to be definitely related with the distance from DMZ. Although unavailable in the present analysis, the incidence data of ROK soldiers guarding DMZ within this county boundary would make the relation between distance from DMZ and the malaria incidence more evident. Kho et al. (
1999a) showed that the malaria cases of the present epidemic are occurring within about 20 km south of the borderline, although higher incidence was observed in areas near DMZ. This study shows the same pattern, but the majority of malaria patients were residents of villages not over 10 km from DMZ. In addition to the distance from DMZ, the degree of topographical ruggedness within the county was related with malaria incidence. The higher incidences were observed in plain areas of the county than in hilly areas. This pattern was repeated every year.
Significant relations of API with distance from DMZ and topograpical ruggedness suggest that the present epidemic is related with flying of infected vector mosquitos from the other side of DMZ. Actually, Lee et al. (
1999) examined the flying distance of
A. sinensis and reported the average distance as 6 km with the maximum as 16 km. Therefore, the flying distance data of local
A. sinensis can explain this skewed geographical incidence pattern.
In Yonchon, the proportion of
A. sinensis among the mosquito population is relatively high throughout the county (
Shim et al., 1997) except for two urbanized towns. In such context, API would not related with distance from DMZ, if the present epidemic is a continuation of the previous endemic malaria in the 1960s (
NMES, 1966); age, sex and geographical distribution of cases would be quite different from this current epidemic.
One of the most important issues of the present epidemic is whether the secondary transmission is occurring or not in the high-risk areas. Up until now, it is technically impossible to determine the place where the vector mosquitoes become naturally infective. Based on the present epidemiologic data, we presume that the infective mosquitoes flying over DMZ are causing most of malaria even if not all of the cases.
Taken together, the findings of the present study strongly support the hypothesis that the contraction of malaria in the high-risk county is related with the flying distance of infected vector mosquitos. The only drawback of this hypothesis is the lack of detailed data on malaria status in the other side of DMZ. Otherwise, it can provide a unique explanation for annually repeating incidence of civilian cases of malaria in the Yonchon-gun.
ADDENDUM
During revising this paper, Dr. Gro Harlem Brundtland, Secretary-General of World Health Organization, after visiting Pyongyang in 17-20 November 2001, said at the press conference in Seoul on 21 November 2001 that 300,000 cases of (vivax) malaria were estimated in Democratic People's Republic of Korea in 2001 and that malaria was especially prevalent in border areas.
ACKNOWLEDGMENTS
We appreciate Professor Keun Young Yoo, Department of Preventive Medicine, Seoul National University College of Medicine for his helps in statistical analysis.
References
- 1. Chai JY. Re-emerging Plasmodium vivax malaria In the Republic of Korea. Korean J Parasitol 1999;37:129-143.
- 2. Kho WG, Jang JY, Hong ST, Lee HW, Lee WJ, Lee JS. Border malaria characters of reemerging vivax malaria in the Republic of Korea. Korean J Parasitol 1999a;37:71-76.
- 3. Kho WG, Park YH, Chung JY, et al. Two new genotypes of Plasmodium vivax circumsporozoite protein found in the Republic of Korea. Korean J Parasitol 1999b;37:265-270.
- 4. Kim MB. Epidemiologic characteristics of malaria in non-malarious area, Jeollabuk-do, Korea in 2000. Korean J Parasitol 2001;39:223-226.
- 5. Lee JS, Kho WG, Lee HW, Seo M, Lee WJ. Current status of vivax malaria among civilians in Korea. Korean J Parasitol 1998;36:241-248.
- 6. Lee JS, Kho WG, Hong ST, et al. Research for the control of Plasmodium vivax in the northern part of Kyonggi-do. Report to Ministry of Health and Welfare. 1999. p. 57-66 (in Korean).
- 7. National Malaria Eradication Service. Malaria pre-eradication programme in Korea. Progress Report, 1961-1965. 1966. Ministry of Health and Social Affairs; p 75.
- 8. Park JW, Son JI, Hur JP, et al. An outbreak of vivax malaria in Republic of Korea in 1999. Korean J Inf Dis 2000;32:335-339.
- 9. Park JW, Kim YA, Yeom JS, Yoo JS, Yang BG, Chal JY. Status of vivax malaria in the Republic of Korea in 2000. Korean J Inf Dis 2001;33:280-284.
- 10. Ree HI. Unstable vivax malaria in Korea. Korean J Parasitol 2000;38:119-138.
- 11. Shim JC, Shin EH, Yang DS, Lee WK. Seasonal prevalence and feeding time of mosquitoes at outbreak regions of domestic malaria in Korea. Korean J Entomol 1997;27:265-277.
Fig. 1Map of Yonchon-gun (county), with the administrative boundaries, demilitarized zone (DMZ, black belt), and the Imjin River (dotted area). Numbers on the map denote: 1, Changnam: 2, Paikhak: 3, Wangjing; 4, Chung; 5, Shinseo; 6, Misan; 7, Kunnam; 8, Yonchon; 9. Chongok; and 10, Chongsan.
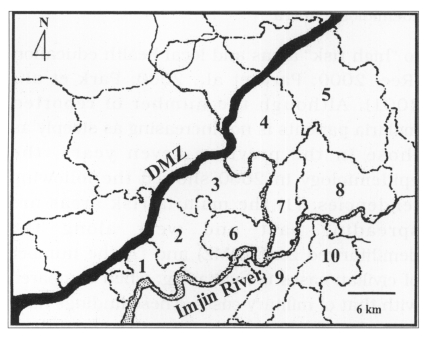
Fig. 2Number of vivax malaria cases reported monthly in Yonchon-gun from 1995 through 2000.
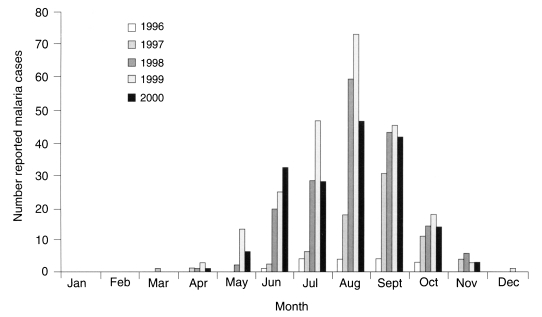
Table 1.Incidence of vivax malaria in civilians living in Yonchon-gun by year and sex
Table 1.
|
Year |
No. of patients
|
Total |
|
Male |
Female |
|
Populationa)
|
27,608 |
26,158 |
53,776 |
|
1995 |
0 |
2 |
2 |
|
1996 |
10 |
4 |
14 |
|
1997 |
42 |
27 |
69 |
|
1998 |
123 |
47 |
170 |
|
1999 |
144 |
80 |
224 |
|
2000 |
101 |
67 |
168 |
|
Total |
420 |
227 |
647 |
Table 2.Annual parasite index by age in Yonchon-gun during 1995-2000
Table 2.
|
Age group (year) |
Populationa)
|
API in
|
Average API |
|
1995 |
1996 |
1997 |
1998 |
1999 |
2000 |
|
< 10 |
6,727 |
0 |
0 |
0 |
0.743 |
1.487 |
0.143 |
0.396 |
|
10-19 |
7,503 |
0.133 |
0.266 |
1.066 |
1.733 |
2.266 |
1.466 |
1.155 |
|
20-29 |
8,940 |
0 |
0 |
0.336 |
2.573 |
2.461 |
0.895 |
1.044 |
|
30-39 |
8,881 |
0 |
0.113 |
0.676 |
3.378 |
4.504 |
4.054 |
2.121 |
|
40-49 |
7,001 |
0.143 |
0.571 |
2.428 |
4.428 |
6.856 |
4.999 |
3.238 |
|
50-59 |
5,891 |
0 |
0.509 |
3.056 |
4.583 |
5.262 |
6.451 |
3.310 |
|
60-69 |
5,295 |
0 |
0.757 |
1.703 |
5.300 |
7.947 |
5.298 |
3.500 |
|
> 70 |
3,528 |
0 |
0 |
2.268 |
3.685 |
3.968 |
3.118 |
2.173 |
|
Total |
53,776 |
0.037 |
0.260 |
1.283 |
3.161 |
4.165 |
3.124 |
2.005 |
Table 3.Annual parasite index by administrative Myeons of Yonchon-gun in 1995-2000
Table 3.
|
Number in map |
Administrative Myeon (M) and Eup (E) |
Populatlonb)
|
API in
|
Average API |
|
1995 |
1996 |
1997 |
1998 |
1999 |
2000 |
|
1 |
Changam(M)a), b)
|
821 |
0 |
1.218 |
6.090 |
15.834 |
20.706 |
8.526 |
8.729 |
|
2 |
Paikhak (M)a), b)
|
3,350 |
0 |
0.896 |
3.582 |
5.672 |
12.239 |
5.970 |
4.726 |
|
3 |
Wangjing(M)a), b)
|
1,547 |
0 |
1.939 |
9.696 |
12.928 |
18.100 |
12.281 |
9.157 |
|
4 |
Chung (M)a), b)
|
244 |
0 |
4.098 |
0 |
12.295 |
12.295 |
4.098 |
5.464 |
|
5 |
Shinseo (M)a)
|
5,155 |
0.388 |
0 |
0.582 |
1.358 |
3.104 |
2.910 |
1.390 |
|
6 |
Misan (M)b)
|
2,165 |
0 |
0.462 |
2.309 |
10.623 |
8.776 |
5.080 |
4.542 |
|
7 |
Kunnam (M)b)
|
4,954 |
0 |
0.807 |
3.835 |
7.267 |
8.478 |
8.478 |
4.811 |
|
8 |
Yonchon (E) |
8,898 |
0 |
0.112 |
0.450 |
2.023 |
3.147 |
3.372 |
1.517 |
|
9 |
Chongok (E) |
20,875 |
0 |
0 |
0.287 |
1.246 |
1.293 |
0.862 |
0.614 |
|
10 |
Chongsan (M) |
5,757 |
0 |
0 |
0 |
0.869 |
0.521 |
0.869 |
0.376 |
Table 4.Annual incidence and API in villages of high-risk Myeons according to distance from DMZ (1998-2000)
Table 4.
|
Myeon No. in Fig. 1/village No. |
Distance from DMZ (km) |
Population |
No, of cases in
|
Average API |
|
1998 |
1999 |
2000 |
|
1-1 |
4 |
71 |
0 |
2 |
1 |
14.085 |
|
1-2 |
6 |
239 |
10 |
8 |
3 |
29.289 |
|
1-3 |
6 |
272 |
0 |
2 |
0 |
2.451 |
|
1-4 |
8 |
243 |
3 |
5 |
3 |
15.089 |
|
2-1 |
5 |
589 |
2 |
13 |
5 |
11.319 |
|
2-2 |
5 |
249 |
3 |
2 |
0 |
6.693 |
|
2-3 |
6 |
149 |
3 |
4 |
2 |
20.134 |
|
2-4 |
7 |
1,158 |
8 |
12 |
11 |
8.923 |
|
2-5 |
9 |
834 |
2 |
8 |
1 |
4.396 |
|
2-6 |
12 |
205 |
1 |
0 |
1 |
3.252 |
|
2-7 |
12 |
105 |
0 |
2 |
0 |
6.349 |
|
3-1 |
7 |
260 |
10 |
12 |
10 |
41.026 |
|
3-2 |
8 |
536 |
0 |
5 |
2 |
4.353 |
|
3-3 |
9 |
166 |
6 |
6 |
3 |
30.120 |
|
3-4 |
12 |
629 |
4 |
5 |
4 |
6.889 |
|
7-1 |
7 |
467 |
9 |
12 |
14 |
24.982 |
|
7-2 |
10 |
1,015 |
13 |
14 |
9 |
11.823 |
|
7-3 |
10 |
881 |
7 |
4 |
8 |
7.189 |
|
7-4 |
11 |
828 |
4 |
9 |
6 |
7.649 |
|
7-5 |
14 |
517 |
1 |
0 |
2 |
1.934 |
|
7-6 |
14 |
874 |
1 |
1 |
3 |
1.907 |
|
7-7 |
14 |
372 |
0 |
1 |
0 |
0.896 |