Abstract
A 46-year old man visited our outpatient clinic with complaint of foreign body sensation in throat after consuming raw freshwater fish 5 days ago. Laryngoscopic examination revealed a motile worm attached on posterior pharyngeal wall. The worm was removed using biopsy forceps under transnasal endoscopy and evidently identified as Clinostomum complanatum after microscopic examination. Patient’s subjective foreign body sensation of throat and hyperemia of laryngeal mucosa remained for approximately 2 weeks post-removal, which were eventually resolved after administration of non-steroidal anti-inflammatory drug and anti-refluxant drug for 2 weeks. Treatment was ended at three weeks since the first visit. C. complanatum infections in humans are rare, and only four cases have been reported in Korea. Symptoms resembling pharyngitis or laryngitis occurs by consumption of raw, infected freshwater fish and treatment is done by mechanically removing the parasite.
-
Key words: Clinostomum complanatum, human case, raw freshwater fish, laryngopharyngitis
INTRODUCTION
Clinostomum complanatum, also commonly known as “yellow grub” is a digenetic trematode. The eggs of these flatworms are released into the water from beaks and throats of definitive hosts such as herons which then infect freshwater fish [
1]. Consumption of raw freshwater fish such as mullet or perch by humans can cause laryngeal or pharyngeal infections, though the incidence is very rare. Since its first report in 1995, only 4 cases have been reported until date in Korea. In the previous reports, patients visited the clinic with sore throat symptoms which developed as early as 3 days after consuming freshwater fish and endoscopic examination evidently revealed parasitic infections at various sites such as pharynx, larynx, and nasopharynx [
2]. The flatworms were endoscopically or surgically removed under sedation and symptoms were eventually resolved.
CASE RECORD
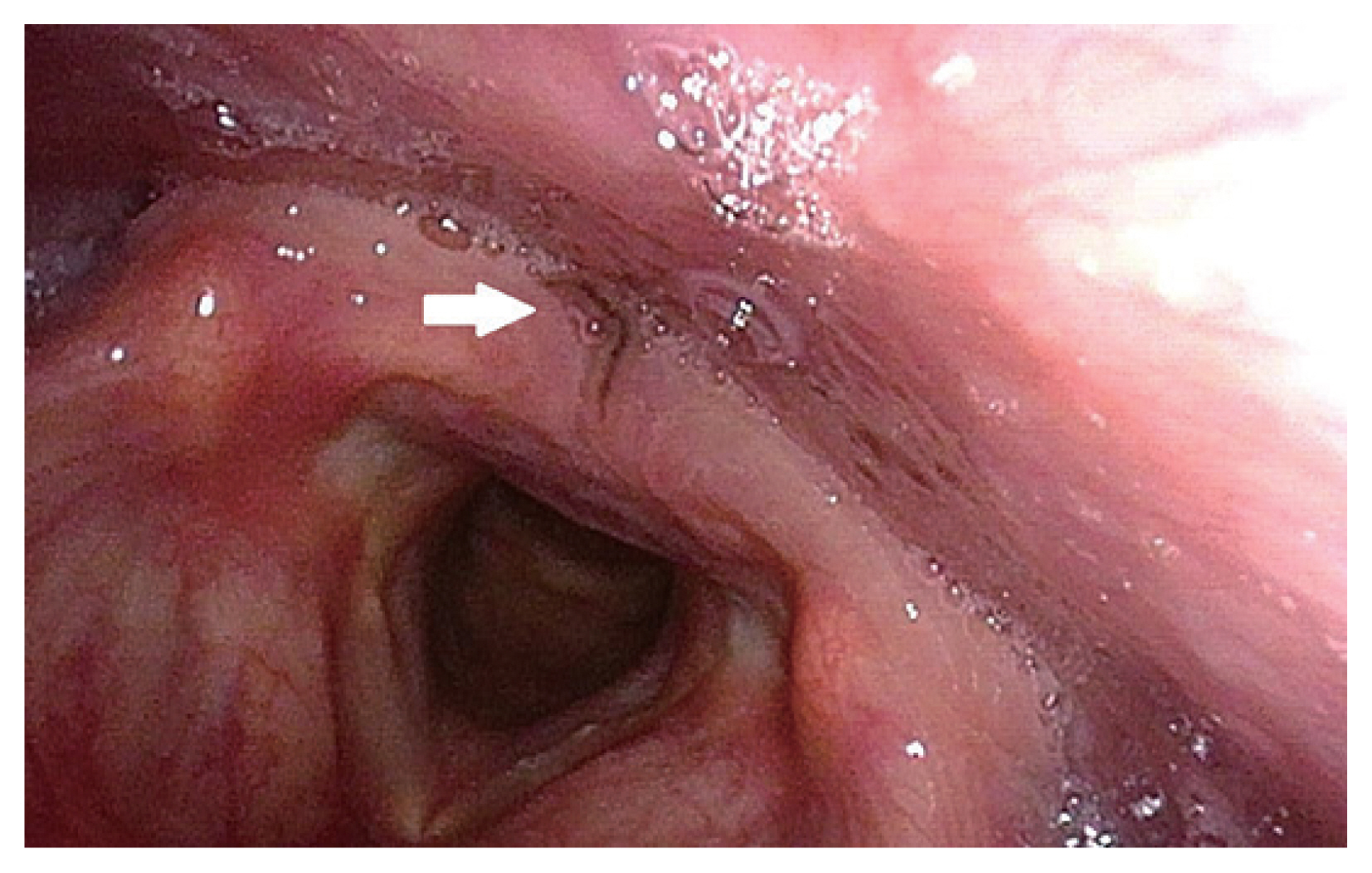
A 46-year old man with no underlying disease was referred to our ENT department from a local clinic for removal of what appeared to be a foreign body (black thread) in pharynx. The patient presented with complaints of foreign body sensation in his throat for the past 2 days and had a history of raw freshwater fish consumption 5 days ago. Close examination under laryngoscopy revealed an approximately 1 cm-sized spontaneously moving organic material located on the posterior pharyngeal wall, just posterior to the interarytenoid mucosa (
Fig. 1). The organism was grasped with biopsy forceps under transnasal flexible endoscopy, in which it was cut into 2 pieces during the process; the obtained specimen was sent for pathologic examination and the remnant piece was suctioned and was unable to be retrieved. Pathologic examination with parasitological consultation identified the organism as an adult parasite worm,
C. complanatum (
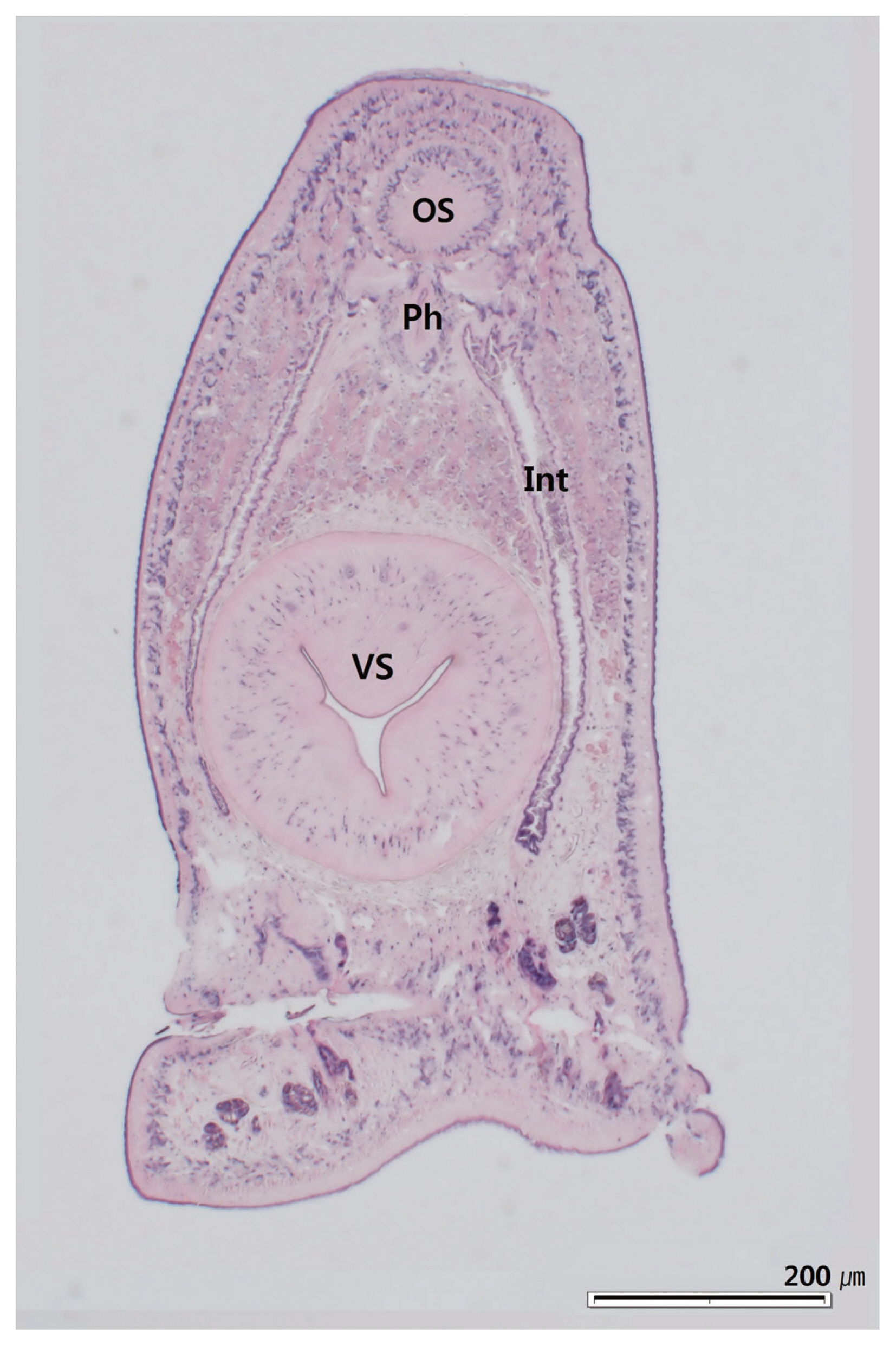
Fig. 2). The retrieved portion of the parasite was prepared and stained with hematoxylin and eosin. Morphological examination of the incomplete piece of
C. complanatum under light microscopy measured 0.95 mm in length and 0.45 mm in width. The oral sucker which was located anteriorly, measured 0.1 mm long and wide, and the ventral sucker, which was located approximately 0.2 mm caudal to the oral sucker, measured 0.3 mm long and wide. According to measurements from previous reports, the ventral sucker of
C. complanatum is located in the anterior third of the body [
3]. Considering these morphological characteristics, the total longitudinal length of this parasite could be assumed to be approximately 2.0 mm long. Intestinal caeca were observed bifurcated on both lateral sides of the parasite in symmetry. The portion of the parasite containing reproductive organs was unable to be retrieved. Considering these morphological characteristics and the anatomical site of infection, the parasite was diagnosed as
C. complanatum. Follow up endoscopy 1 week after the procedure revealed mild hyperemia of the treated site of mucosa which was completely recovered by the second week. Conservative medical treatment with nonsteroidal anti-inflammatory drug and anti-refluxant drug was provided for 2 weeks, and the foreign body sensation was completely resolved by the last follow-up visit.
DISCUSSION
C. complanatum is a digenetic trematode that naturally parasitizes in the throat of piscivorous birds such as herons and egrets, and many species of fresh-water fish are recorded as second intermediate hosts [
3]. Fish-borne trematode infections in humans result from eating raw or undercooked freshwater fish [
4]. Although the general incidence of human parasitic infection is decreasing due to changes in lifestyle and use of chemical fertilizers, infections of food-borne parasites are still observed in areas where people remain to consume raw meat of fish [
5]. Human
C. complanatum infection was first reported by Yamashita in 1938 in Japan, and the first case in Korea was reported by Chung in 1995.
Usually the only symptom is throat discomfort, which occurs several days after consumption of infected fish. This is due to the life cycle of
C. complanatum; when the metacercaria enters the human body, it excysts in the stomach and migrates through the esophagus and attaches to the throat where it matures [
5]. The nutritional source of
C. complanatum is glucose obtained from necrosis of engulfed tissues by the parasite’s oral suckers [
6]. Throat discomfort and petechial hemorrhage of the infected mucosa are usually self-limiting once the parasite is removed.
Infection is diagnosed by laryngoscopic or endoscopic examination, in which the parasite is spotted in various locations such as pharynx, arytenoid, or posterior pharyngeal wall [
5]. To treat the infection, the flatworm is mechanically removed either under local or general anesthesia. Spraying of 8% lidocaine solution can be helpful in inhibiting its motility and eliminating suction to host’s mucosa to safely remove the infection source without damaging surrounding tissues [
7]. Antiparasitic medication is ineffective and upper gastrointestinal endoscopy is recommended to confirm that there is no other residual parasite [
2,
5].
Previous cases reported
C. complanatum infection in various sites such as posterior pharyngeal wall, larynx, and nasopharynx. Except for 1 case of upper pharyngeal infection in which simple otolaryngological removal was able to be done, endoscopic or surgical removal of parasites located in the larynx or nasopharynx required sedation or general anesthesia [
2]. In the present case, transnasal flexible endoscopy was performed to remove the parasite in the larynx, which was performed in the outpatient clinic setting without any sedation or subsequent hospitalization. This office-based procedure allowed safe and complete removal of the foreign body, and was a convenient technique for both the clinician and the patient.
Laryngopharyngitis by C. complanatum infection is a rare occurrence and only a few cases have been reported in Korea. However, the incidence may have been underestimated due to inadequate endoscopic examination in the past. With increasing access to endoscopic examination, the number of reported cases are expected to grow with careful inspection and appropriate suspicion. In areas where rare freshwater fish meat consumption is still a common occurrence, C. complanatum infection should be considered as a possible diagnosis and endoscopic examination and appropriate removal should be promptly done.
Notes
-
CONFLICT OF INTEREST
The authors declare no conflict of interest related to this study.
Fig. 1Motile organism is attached to posterior pharyngeal wall, just posterior to the interarytenoid mucosa (white arrow).

Fig. 2Histological section of head portion of C. complanatum in H&E stain showing oral sucker (OS), pharynx (Ph), intestinal caeca (Int), and ventral sucker (VS).

References
- 1. Song HB, Choi MH, Chung EJ. Human laryngeal infection by Clinostomum complanatum
. Am J Trop Med Hyg 2018;98:7-8.
- 2. Lee GS, Park SW, Kim J, Seo KS, You KW, Chung JH, Moon HC, Hong GY. A case of endoscopically treated laryngopharyngitis resulting from Clinostomum complanatum infection. Korean J Gastroenterol 2017;69:177-180.
- 3. Chung DI, Kong HH, Moon CH. Demonstration of the second intermediate hosts of Clinostomum complanatum in Korea. Korean J Parasitol 1995;33:305-312.
- 4. Sohn WM. Fish-borne zoonotic trematode metacercariae in the Republic of Korea. Korean J Parasitol 2009;47( suppl):103-113.
- 5. Hara H, Miyauchi Y, Tahara S, Yamashita H. Human laryngitis caused by Clinostomum complanatum
. Nagoya J Med Sci 2014;76:181-185.
- 6. Park CW, Kim JS, Joo HS, Kim J. A human case of Clinostomum complanatum infection in Korea. Korean J Parasitol 2009;47:401-404.
- 7. Kitagawa N, Oda M, Totoki T, Washizaki S, Oda M, Kifune T. Lidocaine spray used to capture a live Clinostomum parasite causing human laryngitis. Am J Otolaryngol 2003;24:341-343.
Citations
Citations to this article as recorded by

- The first case of human invasion by Clinostomum complanatum in the European part of Russia
Larisa Ermakova, Sergey Kozlov, Sergey Nagorny, Natalia Golovchenko, Victoria Telicheva, Julia Kiosova, Marina Zotova, Natalia Pshenichnaya
IJID Regions.2024; 11: 100346. CrossRef - Unregulated introduced fish (Perca fluviatilis Linnaeus, 1758) is host to zoonotic parasites in a small Mediterranean island
Anaïs Esposito, Gaël P. J. Denys, Vincent Haÿ, Paul-Jean Agostini, Joséphine Foata, Yann Quilichini
Parasitology Research.2024;[Epub] CrossRef - Genetic Diversity and Population Dynamics of Clinostomum spp. Using Comprehensive Bioinformatics Approaches
Sk Injamamul Islam, Mohamed H. Hamad, Wanarit Jitsamai, Channarong Rodkhum, Piyanan Taweethavonsawat, Mohammed El-Magd
Veterinary Medicine International.2024;[Epub] CrossRef - Yellow grub diseases on two seasonal killifish (Cyprinodontiformes, Rivulidae): a histopathological study
L. Di Cesare, M. M. Montes, M. S. Vargas, C. G. Barbeito, S. E. Plaul
Parasitology Research.2024;[Epub] CrossRef - Can avian flyways reflect dispersal barriers of clinostomid parasites? First evidence from the mitogenome of Clinostomum complanatum
Marlies Monnens, Ali Halajian, D. Tim J. Littlewood, Andrew G. Briscoe, Tom Artois, Maarten P.M. Vanhove
Gene.2023; 851: 146952. CrossRef - Clinostomum complanatum: Anthelmintic potential of curcumin on the infective progenetic metacercarial stage
Lubna Rehman, Rizwan Ullah, Abdur Rehman, M.A. Hannan Khan, Mirza Ahmar Beg, Sobia Wasim, Faiza Farhat, P A Shareef Ahammed, S.M.A. Abidi
Experimental Parasitology.2023; 249: 108514. CrossRef - Case report of laryngeal infection by Clinostomum complanatum 24 days after ingestion of raw fish
Hyun-Gyu Kim, Ji-Hee Han, Ji-Yoon Kwak, Han Kyu Jeon, Sang-Soo Lee, Hyun Jin Kim, Seul Ki Song, Byoung-Kuk Na, Ra-Ri Cha
Medicine.2023; 102(22): e34000. CrossRef - Occurrence of digenean parasites in freshwater snails in the Murrumbidgee catchment area, Australia
Shokoofeh Shamsi, Alice Banfield, Nidhish Francis, Diane P. Barton, Matthew McLellan
Food and Waterborne Parasitology.2023; 32: e00202. CrossRef - Integrative analysis of new Clinostomum metacercariae (Digenea, Clinostomidae) using COI mtDNA and morphology rises the number of lineages found in South American freshwater fishes
M.M. Montes, I. García, J.M. Paredes del Puerto, J.A. Barneche, M. Ibañez Shimabukuro, G.F. Reig Cardarella, S.R. Martorelli, G. Pérez Ponce de León
Journal of Helminthology.2023;[Epub] CrossRef - The Occurrence of Freshwater Fish-Borne Zoonotic Helminths in Italy and Neighbouring Countries: A Systematic Review
Vasco Menconi, Elena Lazzaro, Michela Bertola, Lisa Guardone, Matteo Mazzucato, Marino Prearo, Ewa Bilska-Zajac, Luana Cortinovis, Amedeo Manfrin, Giuseppe Arcangeli, Giorgia Angeloni
Animals.2023; 13(24): 3793. CrossRef - A case of tonsillitis caused by parasitization of Clinostomum complanatum
Sergei S. Kozlov, Larisa A. Ermakova, Vladimir S. Turitsin, Marina A. Zotova
Epidemiology and Infectious Diseases.2023; 28(6): 401. CrossRef - Development of real-time and lateral flow recombinase polymerase amplification assays for rapid detection of Schistosoma mansoni
Silvia Gonçalves Mesquita, Elena Birgitta Lugli, Giovanni Matera, Cristina Toscano Fonseca, Roberta Lima Caldeira, Bonnie Webster
Frontiers in Microbiology.2022;[Epub] CrossRef - Molecular data reveal hidden diversity of the genus Clinostomum (Digenea, Clinostomidae) in Argentina, with the description of a new species from Ardea cocoi (Ardeidae)
Martin Miguel Montes, Jorge Barneche, Luis Pagano, Walter Ferrari, Sergio Roberto Martorelli, Gerardo Pérez-Ponce de León
Parasitology Research.2021; 120(8): 2779. CrossRef - Pathology associated with three newClinostomummetacercariae from Argentina with morphological and DNA barcode identification
M.M. Montes, S.E. Plaul, Y. Croci, M. Waldbillig, W. Ferrari, E. Topa, S.R. Martorelli
Journal of Helminthology.2020;[Epub] CrossRef - A multiplex PCR protocol for rapid differential identification of four families of trematodes with medical and veterinary importance transmitted by Biomphalaria Preston, 1910 snails
Silvia Gonçalves Mesquita, Gabriela Flávia Rodrigues-Luiz, João Luís Reis-Cunha, Mariana Santos Cardoso, Cristiane Lafetá Furtado De Mendonça, Lilian Lacerda Bueno, Ricardo Toshio Fujiwara, Hudson Alves Pinto, Roberta Lima Caldeira, Daniella Castanheira B
Acta Tropica.2020; 211: 105655. CrossRef - Digestive tract trematodiases (invasions caused by intestinal flukes)
S. B. Chuyelov, A. L. Rossina
CHILDREN INFECTIONS.2020; 19(4): 38. CrossRef - Morphological and Molecular Characteristics of Clinostomid Metacercariae from Korea and Myanmar
Eun Jeong Won, Yu Jeong Lee, Moon-Ju Kim, Jong-Yil Chai, Byoung-Kuk Na, Woon-Mok Sohn
The Korean Journal of Parasitology.2020; 58(6): 635. CrossRef - Infection Status with Clinostomum complanatum Metacercariae in Fish from Water Systems of Nakdong-gang (River) in Korea
Woon-Mok Sohn, Byoung-Kuk Na, Shin-Hyeong Cho
The Korean Journal of Parasitology.2019; 57(4): 389. CrossRef - A study of the endohelminths of the European perch Perca fluviatilis L. from the central region of the Danube river basin in Slovakia
Ľudmila Juhásová, Alžbeta Radačovská, Eva Bazsalovicsova, Dana Miklisová, Marcela Bindzárová-Gereľová, Ivica Králová-Hromadová
ZooKeys.2019; 899: 47. CrossRef